Understanding Thyroid Goiter Embolization Techniques
Thyroid Goiter Embolization is a minimally invasive procedure to shrink goiters by blocking their blood supply. At CVI Thyroid Center, we specialize in Thyroid Goiter Embolization, offering a safe, effective alternative to surgery. Using advanced imaging, we precisely target the thyroid, reducing symptoms and improving quality of life. As a trusted service provider, we ensure expert care, personalized treatment, and faster recovery for patients seeking non-surgical thyroid solutions.<br><br>Visit us:- https://cvithyroidcenter.com/


Understanding Thyroid Goiter Embolization Techniques
E N D
Presentation Transcript
Understanding Thyroid Goiter Embolization Techniques www.cvithyroidcenter.com
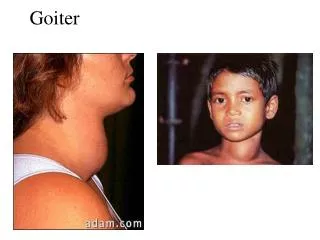
Introduction BRIEFLY DEFINE THYROID GOITER (ABNORMAL ENLARGEMENT OF THE THYROID GLAND). EXPLAIN WHY TREATMENT IS NECESSARY (SYMPTOMS, COSMETIC CONCERNS, COMPRESSION OF NEARBY STRUCTURES). INTRODUCE EMBOLIZATION AS AN EMERGING TECHNIQUE IN GOITER MANAGEMENT.
Anatomy & Function of the Thyroid Gland 2 1 3 Location and structure of the thyroid. Role in hormone production (T3, T4, and their impact on metabolism). Common causes of thyroid goiter (iodine deficiency, nodules, Graves’ disease, etc.).
Conventional Treatments for Thyroid Goiter Medication: Hormone therapy, anti-thyroid drugs. Surgery: Thyroidectomy and its risks. Radiofrequency Ablation (RFA): A newer, minimally invasive approach. Introduce embolization as an alternative technique.
What is Thyroid Goiter Embolization? Embolization is a medical procedure that deliberately blocks blood flow to a specific area, such as a goiter, to reduce its size. By injecting tiny particles into the thyroid's blood vessels, the procedure cuts off its blood supply, causing the goiter to shrink over time. The mechanism involves injecting embolic agents into the thyroid arteries to obstruct blood flow, reducing vascular supply to the thyroid gland. This process induces ischemia, leading to tissue shrinkage or necrosis, which is useful in treating hypervascular thyroid conditions. The goal is to reduce goiter size and relieve symptoms without surgery by using medication, dietary adjustments, and lifestyle changes. Treatments may include iodine supplements for deficiency, thyroid hormone therapy to regulate function, and anti-inflammatory measures to reduce swelling.
Indications for Thyroid Goiter Embolization Best suited for: Large benign goiters are non-cancerous thyroid gland enlargements that may cause swelling and discomfort. Patients who are medically unstable, have severe comorbidities, or high surgical risks are unfit for surgery. Achieve aesthetic improvements without scars through non- invasive or minimally invasive cosmetic treatments. Not suitable for: Malignant thyroid nodules are cancerous growths in the thyroid gland, requiring diagnosis and treatment. Patients experiencing critical imbalances in thyroid hormone levels, leading to serious metabolic complications.
The Embolization Procedure Before the procedure, imaging (CT, MRI, ultrasound) assesses anatomy, and blood tests check health status. Procedure steps: Local anesthesia is a medication that numbs a specific area of the body to block pain during procedures. Catheter insertion via the femoral artery is a procedure to access blood vessels for diagnostics or treatment. The injection of embolic material blocks blood flow to a targeted area, preventing oxygen and nutrient delivery. After the procedure, monitor for mild swelling or pain. Use ice packs, rest, and follow medical advice.
Risks and Limitations Potential risks: Temporary pain or swelling is a short-term discomfort caused by injury, inflammation, or irritation, subsiding soon. Non-target embolization is an uncommon complication where embolic material unintentionally blocks non-target vessels. In some cases, follow-up treatments are needed to ensure full recovery, manage symptoms, or prevent relapse. The long-term effectiveness of this treatment is still being studied, with ongoing evaluations comparing its outcomes to those of surgical interventions.
Case Studies & Research Findings Studies support embolization as an effective treatment for tumors and vascular malformations, often matching or surpassing surgery and RFA in reducing blood loss, hospital stays, and recovery times. As a minimally invasive alternative, it carries fewer complications and speeds up recovery, though long-term efficacy varies. While surgery removes tissue and RFA destroys it, embolization blocks blood flow, causing necrosis. Patients report less pain, faster recovery, and improved quality of life.
Conclusion Thyroid goiter embolization is emerging as a viable alternative to surgery, offering a minimally invasive option with reduced recovery time and complications. Proper patient selection is crucial to ensure optimal outcomes, as not all cases may benefit equally. Identifying ideal candidates enhances success rates and patient satisfaction. Further research and clinical adoption are encouraged to refine techniques, validate long-term efficacy, and expand accessibility for improved patient care.