Download

1 / 184
1.86k likes | 2.66k Views
Diseases of the Skin Appendages. Alopecia areata. Characterized by rapid and complete loss of hair in one , or more often several round or oval patches Usually on the scalp, bearded areas, eyebrows and eyelashes 1-5 cm

E N D
Alopecia areata • Characterized by rapid and complete loss of hair in one , or more often several round or oval patches • Usually on the scalp, bearded areas, eyebrows and eyelashes • 1-5 cm • May progress to total loss of scalp hair – alopecia totalis, or hair loss involving the entire body – alopecia universalis
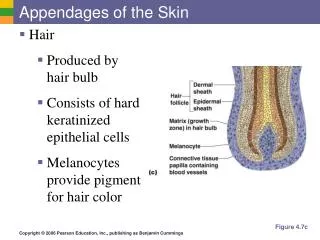
Usually occurs without associated disease However, there is a higher incidence in patients with atopic dermatitis, Down syndrome, LP, LE, thyroiditis, MG and vitiligo Nails may develop uniform pits that may form transverse or longitudinal lines – 10 %
etiology • Cause unknown • Most evidence points toward its being an autoimmune disease mediated by the cellular arm and modified by genetic factors • 25% report family history • Patients with early onset, severe, familial clustering alopecia areata have a unique and highly significant association with HLA antigens DR4, DR11, and DQ7
histology • In early disease there is a helper T-cell lymphocytic infiltrate in the peribulbar area of anagen or early catagen follicles • DDX • Tinea capitis, early lupus erythematosis, syphilis, congenital triangular alopecia, alopecia neoplastica and trichotillomania
TX • Intralesional injections of corticosteroid suspensions, q 6 weeks • High-strength topical steroid creams • Anthralin • Minoxidil alone or combined therapy
Spontaneous recovery is extremely common • Tendency is for spontaneous recovery in patients who are post pubertal at onset • Predictors of poor prognosis include the presence of atopic dermatitis, childhood onset, widespread involvement, ophiasis, duration of longer than 5 years, and onychodystrophy
Telogen effluvium • Early and excessive loss of normal club hairs from normal resting follicles in the scalp • Loss results from traumatization of the normal hair by some stimulus, such as surgery, parturition, fever, drugs, or traction which precipitates the anagen phase into catagen and telogen phases • Follicle is not diseased and inflammation is absent
“lots of hairs coming out by the roots” • Loss is diffuse and only infrequently causing clinically perceptible thinning of hair • Normal telogen count is below 10% • Can be estimated by the pull test • Grasping 40 hairs firmly between thumb and forefinger, followed by a slow pull • Greater than 4-6 club hairs is abnormal
100 – 150 hairs lost daily • 150 – 400 lost in telogen effluvium
Postpartum telogen effluvium • Between 2-6 months postpartum • Diffuse pattern, may be first noted over anterior scalp • May continue for another 2-6 months
Drug induced telogen effluvium • Amphetamines, aminosalicyclic acid, bromocriptine, captopril, coumarin, carbamazepine, cimetidine, danazol, enalapril, lithium carbonate, levodopa, metyrapone, metoprolol, propranolol, pyridostigimine and trimethadione
TX • No specific therapy • In the majority of cases it will stop spontaneously within a few months and the hair will regrow • Chronic form may occur • 5% minoxidil solution • education
Anagen effluvium • Seen frequently following the administration of cancer chemotherapeutic agents, such as antimetabolites, alkylating agents, and mitotic inhibitors • Only anagen hairs are involved • With cessation of the drug the follicle resumes normal activity within a few weeks • Process being entirely reversible • Topical minoxidil may decrease the period of baldness by an average of 50 days
Androgenetic alopeciamale-pattern baldness • Shows itself during the twenties of early thirties by gradual loss of hair, chiefly from the vertex and frontotemporal regions • Several patterns of this type occur • Most frequent is the biparietal recession with loss of hair on the vertex • Rate varies
The exact mechanisms responsible for androgenetic alopecia are still unknown, however, there is no doubt that inherited factors and the effect of androgens on the hair follicle are most responsible • Pathogenesis involves lengthening of telogen phase and shortening of the anagen phase
TX • Minoxidil • 2% and 5% • Indefinite treatment to maintain a response • 1/3 cases grow cosmetically useful hair • Finasteride • Effective in preventing further hair loss and in increasing the hair counts • Hair transplantation
Androgenetic alopecia in women • Generally diffuse hair loss throughout the midscalp, sparing the frontal hairline except for slight recession • The midline part is an important clinical clue to the diagnosis, revealing this central thinning by the appearance of the “Christmas tree pattern” • The cause is now believed to be a genetic predisposition in combination with an excessive androgen response
TX • Topical minoxidil 2%
trichotillomania • A neurotic practice of plucking or breaking hair from the scalp or eyelashes • Usually localized but may be widespread • Areas of alopecia characteristically contain hairs of various lengths • Seen mostly in girls under 10, may also be seen in boys and adults
It has been suggested that one ask the child not if but rather how the removal is done • Shave 3 X 3 cm area and watch the hair regrow normally. Hairs in this ‘skin window” will be too short for plucking • Biopsy – high number of catagen hairs, pigmentary defects and casts, trichomalacia and heorrhage
May be a manifestation of obsessive-compulsive disorder May be assoc with depression or anxiety TX – psychotherapy, behavioral therapy or an appropriate psychopharmacologic medication fluoxetine trichotillomania
Hot comb alopecia • Develops characteristically on the crown and spreads peripherally to form a large oval area of partial hair loss • Initially reported in black women who straightened their hair with hot combs • The hot petrolatum used with the iron causes thermal damage to the hair follicle
Pseudopelade of Brocq(alopecia cicatrisata) • A rare form of scarring alopecia • Destruction of the hair follicle produces multiple, round, oval, or irregularly shaped, hairless, cicatricial patches of varying sizes • Coin sized and white or slightly pink colored with a smooth, shiny, marble like or ivory, atrophic, “onion skin” surface
Inflammation is completely absent • No pustules, crusts, or broken off hairs • Insidious onset • Permanent and slowly progressive • Topical and intralesional steroids, long-term TCN in antiinflammatory doses- not often successful
Traction alopecia • Occurs from prolonged tension on the hair • Either from the hair tightly braided or in a ponytail
Pressure alopecia • Occurs frequently on the occipital areas of babies lying on their backs • In adults it is seen most often after prolonged pressure on the scalp during general anesthesia, with the head fixed in one position • Most likely due to pressure induced ischemia
Loose anagen syndrome • Disorder in which anagen hairs may be pulled from the scalp with little effort • Occurs mostly in blonde girls • Improves with age
Alopecia syphilitica • May have a typical moth-eaten appearance on the occipital scalp, a generalized thinning, or a combination of the two • Eyebrows and lashes, and other body hair may be involved • May be the first sign of a syphilis infection
Follicular mucinosis(alopecia mucinosa) • Most commonly occurs on the scalp or beard area • Manifest as deposition of mucin in the outer root sheath and sebaceous glands • Inflammatory reaction produces alopecia, and at times hypopigmentation • Primary cases occur either as localized lesions of the head or neck typically resloving within a year
Follicular mucinosis(alopecia mucinosa) • More generalized lesion have a longer course • Young people are primarily affected • A secondary type – associated with cutaneous T-cell lymphoma, usually more widespread and in older persons
Inflammatory alopecia • May be seen in lichen simplex chronicus and various eczematous changes on the scalp, including kerion • DLE, lichen planopilaris, sarcoidosis, and folliculitis decalvans are the commonest inflammatory causes of cicatricial alopecia
Vascular or neurologic alopecia • Most often of the lower extremities • May be seen in diabetes mellitus or atherosclerosis
Endocrinologic alopecia • May occur in various endocrinologic disorders • Hypothyroidism – hair becomes dry, brittle, coarse and sparse • Hyperthyroidism – hair becomes extremely fine and sparse • Some women develop telogen effluvium 2-4 months after discontinuing anovulatory agents