Download
1 / 4
40 likes | 55 Views
Vios Compounding Pharmacy provides a full line of compound medications, customized according to your physician's orders.

E N D
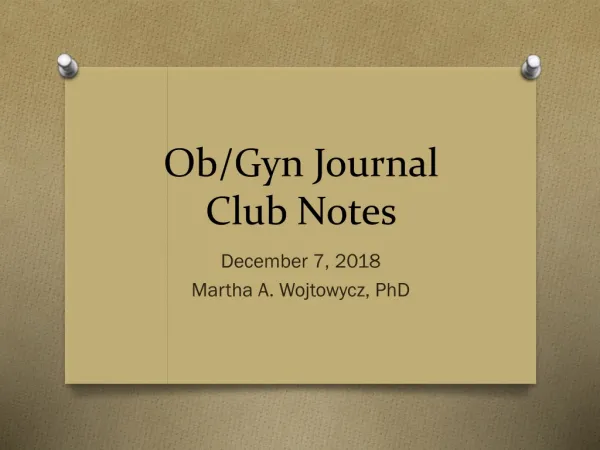
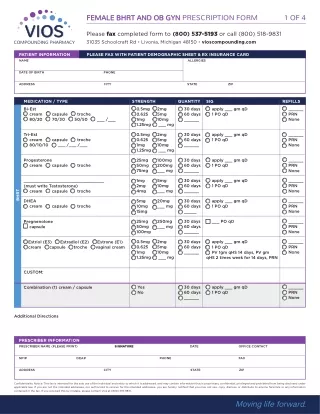
FEMALE BHRT AND OB GYN PRESCRIPTION FORM 1 OF 4 Please fax completed form to (800) 537-5193 or call (800) 518-9831 31035 Schoolcraft Rd • Livonia, Michigan 48150 • vioscompounding.com PATIENT INFORMATION PLEASE FAX WITH PATIENT DEMOGRAPHIC SHEET & RX INSURANCE CARD NAME ALLERGIES DATE OF BIRTH PHONE ADDRESS CITY STATE ZIP MEDICATION / TYPE Bi-Est cream capsule troche 80/20 70/30 50/50 ___ /___ STRENGTH 0.5mg 0.625 1mg 1.25mg QUANTITY 30 days 60 days ______ SIG apply ___ gm qD 1 PO qD REFILLS ______ PRN None 2mg 5mg 10mg ___ mg 0.5mg 0.625 1mg 1.25mg 2mg 5mg 10mg ___ mg 30 days 60 days ______ Tri-Est cream capsule troche 80/10/10 ___ /___ /___ apply ___ gm qD 1 PO qD ______ PRN None 25mg 50mg 75mg 100mg 200mg ___ mg 30 days 60 days ______ Progesterone cream capsule troche apply ___ gm qD 1 PO qD ______ PRN None 1mg 2mg 4mg 5mg 10mg ___ mg 30 days 60 days ______ apply ___ gm qD 1 PO qD ______ PRN None ________________________________ (must write Testosterone) cream capsule troche BHRT 5mg 10mg 15mg 20mg ___ mg 30 days 60 days _____ apply ___ gm qD 1 PO qD ______ PRN None DHEA cream capsule troche 25mg 50mg 100mg 250mg ___ mg 30 days 60 days ______ ______ PRN None ___ PO qD Pregnenolone capsule 0.5mg 0.625 1mg 1.25mg 2mg 5mg 10mg ___ mg 30 days 60 days ______ ______ PRN None apply ___ gm qD 1 PO qD PV 1gm qHS 14 days, PV gm qHS 2 times week for 14 days, PRN Estriol (E3) Estradiol (E2) Estrone (E1) cream capsule troche vaginal cream CUSTOM: 30 days 60 days ______ apply ___ gm qD 1 PO qD ______ PRN None Yes No Combination (1) cream / capsule Additional Directions PRESCRIBER INFORMATION SIGNATURE PRESCRIBER NAME (PLEASE PRINT) DATE OFFICE CONTACT NPI# DEA# PHONE FAX ADDRESS CITY STATE ZIP Confidentiality Notice: This fax is intended for the sole use of the individual and entity to which it is addressed, and may contain information that is proprietary, confidential, privileged and prohibited from being disclosed under applicable law. If you are not the intended addressee, nor authorized to receive for the intended addressee, you are hereby notified that you may not use, copy, disclose or distribute to anyone facsimile or any information contained in the fax. If you received this by mistake, please contact Vios at (800) 518-9831.
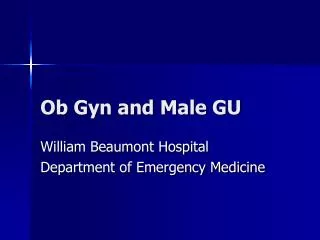
FEMALE BHRT AND OB GYN PRESCRIPTION FORM 2 OF 4 Please fax completed form to (800) 537-5193 or call (800) 518-9831 31035 Schoolcraft Rd • Livonia, Michigan 48150 • vioscompounding.com PATIENT INFORMATION PLEASE FAX WITH PATIENT DEMOGRAPHIC SHEET & RX INSURANCE CARD NAME ALLERGIES DATE OF BIRTH PHONE ADDRESS CITY STATE ZIP MEDICATION / TYPE Naltrexone LDN (for migraines) STRENGTH 1.5mg 3mg 4.5mg QUANTITY 30 days 60 days ______ SIG Take 1 PO QHS REFILLS ______ PRN None GHRH & SEXUAL ENHANCEMENT 30gm 1.2% ______ PRN None Gabapentin (for migraines) Apply 1mL to wrist ______ PRN None 60 10iu 50iu Oxytocin (trochee) Completely dissolve 1 trochee under tongue BID ______ PRN None 15gm Sildenafil 2.5%, Arginine 6%, Pentoxifylline 5% with ______0.4% Libido Cream ________________________________ (must write Testosterone) PRN PV prior to intercourse NAUSEA / VOMITING Meclizine 2.5% (cream) ______ PRN None 30gm Apply 1gm to inner wrist q4-5° PRN Ondansetron 8mg/ml (gel) ______ PRN None 30gm Apply 1mL to inner wrist TID PRN PREGNANCY HEMORRHOIDS Hydrocortisone 2%, Pramoxine 1% ______ PRN None 12 20 30 60 Insert 1 SUPP PR TID PRN ANAL FISSURE Nitroglycerin 0.13%, Lidocaine 5% ______ PRN None 30gm Apply sparingly 4-6° PRN to affected area NIPPLE SORENESS Mupirocin 2%, Betamethasone 0.1%, Miconazole 2% ______ PRN None 30gm Apply sparingly after each feeding Additional Directions PRESCRIBER INFORMATION SIGNATURE PRESCRIBER NAME (PLEASE PRINT) DATE OFFICE CONTACT NPI# DEA# PHONE FAX ADDRESS CITY STATE ZIP Confidentiality Notice: This fax is intended for the sole use of the individual and entity to which it is addressed, and may contain information that is proprietary, confidential, privileged and prohibited from being disclosed under applicable law. If you are not the intended addressee, nor authorized to receive for the intended addressee, you are hereby notified that you may not use, copy, disclose or distribute to anyone facsimile or any information contained in the fax. If you received this by mistake, please contact Vios at (800) 518-9831.
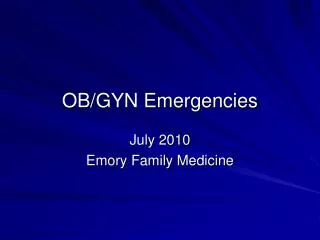
FEMALE BHRT AND OB GYN PRESCRIPTION FORM 3 OF 4 Please fax completed form to (800) 537-5193 or call (800) 518-9831 31035 Schoolcraft Rd • Livonia, Michigan 48150 • vioscompounding.com PATIENT INFORMATION PLEASE FAX WITH PATIENT DEMOGRAPHIC SHEET & RX INSURANCE CARD NAME ALLERGIES DATE OF BIRTH PHONE ADDRESS CITY STATE ZIP MEDICATION / TYPE Estriol vaginal cream STRENGTH 0.5mg 0.625 1mg 1.25mg QUANTITY 30gm 60gm SIG PV 1gm qHS 14 days, PV 1gm qHS 2 time week 14 days, PRN REFILLS ______ PRN None Estradiol 2mg 5mg 10mg ___ mg VAGINAL DRYNESS 0.5mg / 1mg / 1mg /gm 30gm 60gm PV 1gm qHS ______ PRN None HLA / Vitamin E / Vitamin A 200mg ______ PRN None 7 days 14 days 28 days Insert 1 SUPP PV qD Fluconazole ______ PRN None 7 days 14 days 28 days 600mg Insert 1 SUPP PV qD Boric Acid YEAST ______ PRN None 30gm Metronidazole 125mg/ml, Nystatin 25,000u/ml 1gm PV HS x 5 night Bacterial Vaginosis ______ PRN None PV SUPP 12 18 6.25mg Imiquimod ______ PRN None 30 caps 500mg Tetracycline ANTIBOIOTICS ______ PRN None 30 caps 100mg Doxycycline ______ PRN None 30 caps 6mg Erythromycin Additional Directions PRESCRIBER INFORMATION SIGNATURE PRESCRIBER NAME (PLEASE PRINT) DATE OFFICE CONTACT NPI# DEA# PHONE FAX ADDRESS CITY STATE ZIP Confidentiality Notice: This fax is intended for the sole use of the individual and entity to which it is addressed, and may contain information that is proprietary, confidential, privileged and prohibited from being disclosed under applicable law. If you are not the intended addressee, nor authorized to receive for the intended addressee, you are hereby notified that you may not use, copy, disclose or distribute to anyone facsimile or any information contained in the fax. If you received this by mistake, please contact Vios at (800) 518-9831.
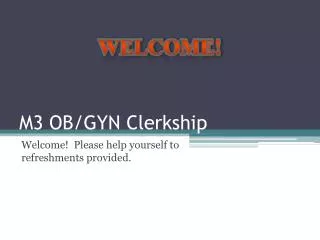
FEMALE BHRT AND OB GYN PRESCRIPTION FORM 4 OF 4 Please fax completed form to (800) 537-5193 or call (800) 518-9831 31035 Schoolcraft Rd • Livonia, Michigan 48150 • vioscompounding.com PATIENT INFORMATION PLEASE FAX WITH PATIENT DEMOGRAPHIC SHEET & RX INSURANCE CARD NAME ALLERGIES DATE OF BIRTH PHONE ADDRESS CITY STATE ZIP MEDICATION / TYPE Libido Cream STRENGTH Sildenafil 2.5%, Arginine 6%, Pentoxifylline 5% QUANTITY 15gm SIG PRN PV prior to intercourse REFILLS ______ PRN None Lidocaine 5%, Diazepam 1% ______ PRN None 30gm 60gm 1gm PV q 6° PRN pain Vulvodynia Cream SEXUAL HEALTH ______ PRN None Amitriptyline 2%, Baclofen 2%, Gabapentin 5% 30gm Apply 0.5gms on vulva upto 3 times daily Vulvodynia Cream Vaginal Cream Option to add Lidocaine ______ PRN None 30gm Apply 1mL to wrist 1.2% Gabapentin (for migraines) ______ PRN None QTY 30 5gm 10gm 20gm Insert 1 vaginally every 4 to 6 hours PRN INTERSTITAL CYSTITIS Diazepam Vaginal Suppositories Additional Directions PRESCRIBER INFORMATION SIGNATURE PRESCRIBER NAME (PLEASE PRINT) DATE OFFICE CONTACT NPI# DEA# PHONE FAX ADDRESS CITY STATE ZIP Confidentiality Notice: This fax is intended for the sole use of the individual and entity to which it is addressed, and may contain information that is proprietary, confidential, privileged and prohibited from being disclosed under applicable law. If you are not the intended addressee, nor authorized to receive for the intended addressee, you are hereby notified that you may not use, copy, disclose or distribute to anyone facsimile or any information contained in the fax. If you received this by mistake, please contact Vios at (800) 518-9831. Reset All Fields