Download
1 / 18
180 likes | 324 Views
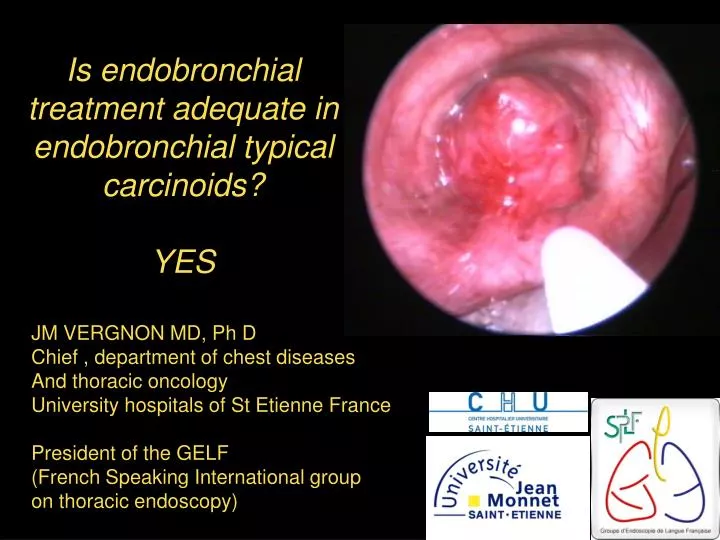
Is endobronchial treatment adequate in endobronchial typical carcinoids? YES. JM VERGNON MD, Ph D Chief , department of chest diseases And thoracic oncology University hospitals of St Etienne France President of the GELF (French Speaking International group on thoracic endoscopy).

E N D
Is endobronchial treatment adequate in endobronchial typical carcinoids?YES JM VERGNON MD, Ph D Chief , department of chest diseases And thoracic oncology University hospitals of St Etienne France President of the GELF (French Speaking International group on thoracic endoscopy)
The carcinoid tumors are neuro-endocrine tumors. several classifications: OMS 1981 3 types: typical, atypical and small cell lung cancer Warren et Gould 1985 4 types Travis 1991 4 types: typical, atypical, large cell NE carcinoma and small cell lung cancer. Carcinoids are rare tumors (1 to 2% of all bronchial tumors)
typical carcinoid: >5 mm, without necrosis,<2 mitoses on 2 mm2
Atypical carcinoid : mitoses ≥ 2 on 2 mm2 and/or focal necrosis
Location et aspect In central airways in 70% of cases, and more frequently in the right side (61%) (Hage) The tumor can be strictly endoluminal like a polyp or with an « iceberg » shape through the bronchial wall Biopsies are often « bleeding » and cytological analysis non contributive.. Well limited tumor in typical type
Location and aspect (2) The aspect is less limited with infiltrative component in atypical carcinoids
Local and mediastinal extension Extension beyond the bronchial wall assessed on CT scan, in depth biopsies ou echoendoscopy Node extension 8-10% N1,3% N2 for typical carcinoids, 27% N1,14% N2 et 14% N3 for atypical carcinoids Metastatic extension for atypical carcinoids
Conventional treatment and prognosis Conventional surgery: lobectomy or more for atypical carcinoids Mediastinal curage +++ Limited surgery (sleeve resection) for typical carcinoids In typical carcinoids : the prognosis is not clearly associated with node invasion. (Hage R et al. Ann Surg Oncol 2003,Ducrocq X, Ann Thorac surg. 1998) Hage R et al. Ann Surg Oncol 2003
Interventional bronchoscopy role large sampling to assess the best classification of carcinoids palliative intent: Debulking treatment hemoptysis control.
Interventional bronchoscopy role Neo-adjuvant therapy Post-obstructive pneumonia drainage Better analysis of tumor limits for minimal surgical resection Curative intent on highly selected patients with typical carcinoids .
Conditions to propose curative bronchoscopic resection Only typical carcinoids strictly endoluminal tumors Tumor accessible with the bronchoscopic tool (rigid or flexible) Thin basis (< 1,5 cm2) Without enlarged lymph nodes on CT scan. Less than 5 cm3 5 similar studies: Sutedja T.: Chest 1995 on 11 patients Van Boxem T.: Journal Thorac Cardiovasc Surg 1998 on 19 patients Cavaliere S.: Journal of Bronchology 2002 on 38 patients (47 in 2005) Luckraz H.: Journal Thorac Cardiovasc Surg 2006 on 28 patients Our team, Bertoletti L.Chest 2006 on 18 patients
Patient selection For S Cavaliere: 47/176 typical carcinoids (27%) For our team 14/29 typical carcinoids referred for resection
Treatment methods YAG laser coagulation, mechanical resection, laser coagulation and sterilization of the basis (Cavaliere) YAG laser coagulation,(or HF electrocautery), mechanical resection and cryotherapy of the basis (St Etienne and Montreal) Mechanical resection and as needed diathermy for Luckraz Van Boxem: HF electrocautery, YAG laser or photodynamic therapy
ENDOSCOPIA RESPIRATORIA SPEDALI CIVILI - BRESCIA
Results T van Boxem: cure 14/19 at 29 months. Surgery proposed for the others due to a remaining tumor. S Cavaliere: only 1 recurrence on 47 patients ,treated with lobectomy. Median follow-up: 38 months. L Bertoletti (St Etienne): 1 local recurrence on 18 patients, 7 years after, treated by lobectomy. Median follow-up : 44.5 mois H Luckraz: mean follow-up 8.8 years (105. 6 months) 1 local recurrence at 80 months, treated by lobectomy. despite the lack of mediastinal curage, no mediastinal recurrence has been observed in these series.
Endoluminal tumor Tumor resection (large Biopsies) Typical carcinoid Atypical carcinoid CT scan ±Echoendoscopy beyond the lumen or N+ Surgical Resection ± th. Bronchoscopy To spare lung parenchyma Resection margins 5mm Mediastinal curage endoluminal Tumor < 5cm3 Central airways N0 NO YES Flexible bronchoscopy + CT scan Each 6 months ,2 years then 1 per year : 5 years Then, on demand only Recurrence T. Bronchoscopy « curative »