Download
1 / 8
110 likes | 424 Views
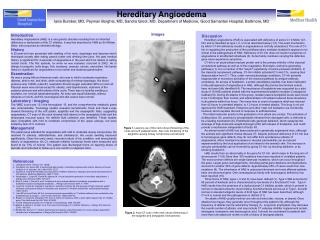
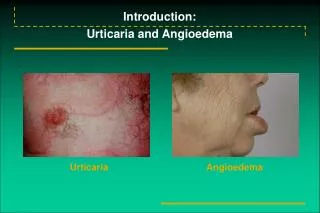
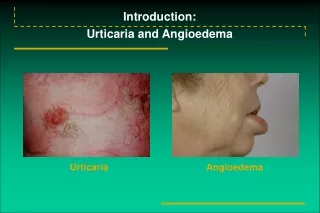
Angioedema. Overview. Self-Limited, subcutaneous edema resulting from increased vascular permeability Dilation of venules and capillaries Different from urticaria Limited to the superficial dermis Generally resolves over 24-48 hours Mast Cell / Kinin related etiologies

E N D
Overview • Self-Limited, subcutaneous edema resulting from increased vascular permeability • Dilation of venules and capillaries • Different from urticaria • Limited to the superficial dermis • Generally resolves over 24-48 hours • Mast Cell / Kinin related etiologies • Involvement of the lips, pharynx and bowel common (potentially life-threatening) • Treated with CCS and H1/H2 blockers • FFP has been used in C1-Inh deficiency
Etiology • Immunologic / IgE mediated • elicited by foods, additives, drugs, transfusions, insect bites and infection • Release of vasoactive mediators from mast cells • Urticaria and pruritis • Hereditary and Acquired (non-mast cell) • Bradykinin and complement-mediated increases in vasc perm. • ACE-I or NSAID
Ace-Inhibitors • ACE (Kininase II) degrades bradykinin • Vasodilator • ACE-I results in inc levels bradykinin • Vasc B-2 rec’s for vasodilation, inc perm, inc NO • Not related to ACE-I induced cough • Pts with genetic deficiencies in bradykinin degradation could be at higher risk • 0.1-0.7% of patients tx with ACE-I • Intestinal edema may develop • Sudden onset abdom pain, vomiting and diarrhea
ACE-I • 50% of cases occur within 1 week of tx • Others may occur years later • Class specific • ARB’s - have been linked to episodes of angioedema • 2 of 26 pts with ACE-I induced angioedema persisted with an ARB and resolved with its withdrawal • Switch with caution
Hereditary/Acquired • Kinin-mediated angioedema that may be unmasked with use of ACE-I • C1-Inh deficiency (level or fx) - Inc BKinin • Normally fx to degrade C1 and prevent excessive complement activation • Dec levels of C1, C2, C4 • Acquired- malignancy or auto-antibodies (older onset)
Summary • Angioedema is potentially life-threatening • Associated pruritis and hives points to anaphylaxis • Absence of pruritis and hives think ACE-I and/or C1-Inh deficiency • PMHx, FHx, Malignancy • Use caution when switching from an ACE-I to an ARB