Download
1 / 20
290 likes | 921 Views
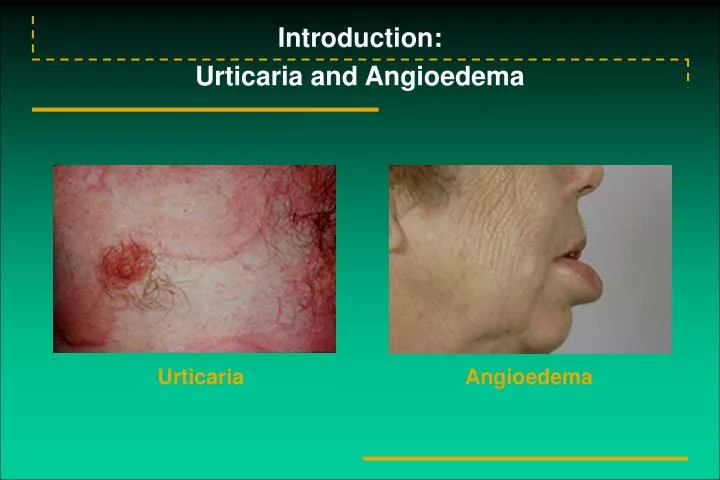
Introduction: Urticaria and Angioedema. Urticaria. Angioedema. Etiology of Urticarial Reactions: Allergic Triggers. Acute Urticaria Drugs Foods Food additives Viral infections hepatitis A, B, C Epstein-Barr virus Insect bites and stings

E N D
Introduction:Urticaria and Angioedema • Urticaria • Angioedema
Etiology of Urticarial Reactions:Allergic Triggers • Acute Urticaria • Drugs • Foods • Food additives • Viral infections • hepatitis A, B, C • Epstein-Barr virus • Insect bites and stings • Contactants and inhalants (includes animal dander and latex) • Chronic Urticaria • Physical factors • cold • heat • dermatographic • pressure • solar • Idiopathic
Role of Mast Cells in Chronic Urticaria:Lower Threshold for Histamine Release • Release threshold decreased by: • Cytokines & chemokines in the cutaneous microenvironment • Antigen exposure • Histamine-releasing factor • Autoantibody • Psychological factors Cutaneous mass cell • Release threshold increased by: • Corticosteroids • Antihistamines • Cromolyn (in vitro)
An Autoimmune Basis for Chronic Idiopathic Urticaria: Antibodies to IgE
Initial Workup of Urticaria • Patient history • Sinusitis • Arthritis • Thyroid disease • Cutaneous fungal infections • Urinary tract symptoms • Upper respiratory tract infection (particularly important in children) • Travel history (parasitic infection) • Sore throat • Epstein-Barr virus, infectious mononucleosis • Insect stings • Foods • Recent transfusions with blood products (hepatitis) • Recent initiation of drugs • Physical exam • Skin • Eyes • Ears • Throat • Lymph nodes • Feet • Lungs • Joints • Abdomen
Laboratory Assessment for Chronic Urticaria • Possible tests for selected patients • Stool examination for ova and parasites • Blood chemistry profile • Antinuclear antibody titer (ANA) • Hepatitis B and C • Skin tests for IgE-mediated reactions • Initial tests • CBC with differential • Erythrocyte sedimentation rate • Urinalysis • RAST for specific IgE • Complement studies: CH50 • Cryoproteins • Thyroid microsomal antibody • Antithyroglobulin • Thyroid stimulating hormone (TSH)
Histopathology • Group 2: • Polymorphous perivascular infiltrate • Neutrophils • Eosinophils • Mononuclear cells • Group 3: • Sparse perivascular lymphocytes
Urticaria Associated With Other Conditions • Collagen vascular disease (eg, systemic lupus erythematosus) • Complement deficiency, viral infections (including hepatitis B and C), serum sickness, and allergic drug eruptions • Chronic tinea pedis • Pruritic urticarial papules and plaques of pregnancy (PUPPP) • Schnitzler’s syndrome
H1-Receptor Antagonists: Pros and Cons for Urticaria and Angioedema • First-generation antihistamines (diphenhydramine and hydroxyzine) • Advantages: Rapid onset of action, relatively inexpensive • Disadvantages: Sedating, anticholinergic • Second-generation antihistamines (astemizole, cetirizine, fexofenadine, loratadine) • Advantages: No sedation (except cetirizine); no adverse anticholinergic effects; bid and qd dosing • Disadvantages: Prolongation of QT interval; ventricular tachycardia (astemizole only) in a patient subgroup
Four-week Treatment Period:Fexofenadine HCl Mean Pruritus Scores/Mean Number of Wheals/Mean Total Symptom Scores
Treatment of Urticaria: Pharmacologic Options • Antihistamines, others • First-generation H1 • Second-generation H1 • Antihistamine/decongestant combinations • Tricyclic antidepressants (eg, doxepin) • Combined H1 and H2 agents • Beta-adrenergic agonists • Epinephrine for acute urticaria (rapid but short-lived response) • Terbutaline • Corticosteroids • Severe acute urticaria • avoid long-term use • use alternate-day regimen when possible • Avoid in chronic urticaria (lowest dose plus antihistamines might be necessary) • Miscellaneous • PUVA • Hydroxychloroquine • Thyroxine
Atopic Dermatitis: Acute, Subacute, and Chronic Lesions • Acute Cutaneous Lesions • Erythematous, intensely pruritic papules and vesicles • Confined to areas of predilection • cheeks in infants • antecubital • popliteal • Subacute Cutaneous Lesions • Erythema excoriation, scaling • Bleeding and oozing lesions • Chronic Lesions • Excoriations with crusting • Thickened lichenified lesions • Postinflammatory hyperpigmentation • Nodular prurigo
Immune Response in Atopic Dermatitis • Markedly elevated serum IgE levels • Peripheral blood eosinophilia • Highly complex inflammatory responses > IgE-dependent immediate hypersensitivity • Multifunctional role of IgE (beyond mediation of specific mast cell or basophil degranulation) • Cell types that express IgE on surface • monocyte/macrophages • Langerhans’ cells • mast cells • basophils
Atopic Dermatitis:Tests to Identify Specific Triggers • Skin prick testing for specific environmental and/or food allergens • RAST, ELISA, etc, to identify serum IgE directed to specific allergens in patients with extensive cutaneous involvement • Tzanck smear for herpes simplex • KOH preparation for dermatophytosis • Gram’s stain for bacterial infections • Culture for antibiotic sensitivity for staphylococcal infection; supplement with bacterial cultures • Cultures to support tests bacterial, viral, or fungal
Topical Corticosteroids • Ranked from high to low potency in 7 classes • Group 1 (most potent): betamethasone dipropionate 0.05% • Group 4 (intermediate potency): hydrocortisone valerate 0.2% • Group 7 (least potent): hydrocortisone hydrochloride 1% • Local side effects: Development of striae and atrophy of the skin, perioral dermatitis, rosacea • Systemic effects: Depend on potency, site of application, occlusiveness, percentage of body covered, length of use • May cause adrenal suppression in infants and small children if used long term
Antihistamines and Other Treatments • Standard Treatment • Oral antihistamines to relieve itching • Moisturizer to minimize dry skin • Topical corticosteroids • Hard-to-manage Disease • Antibiotics • Coal tar preparations (antipruritic and anti-inflammatory) • Wet dressings and occlusion • Systemic corticosteroids • UV light therapy • Hospitalization