Download
1 / 36
400 likes | 764 Views
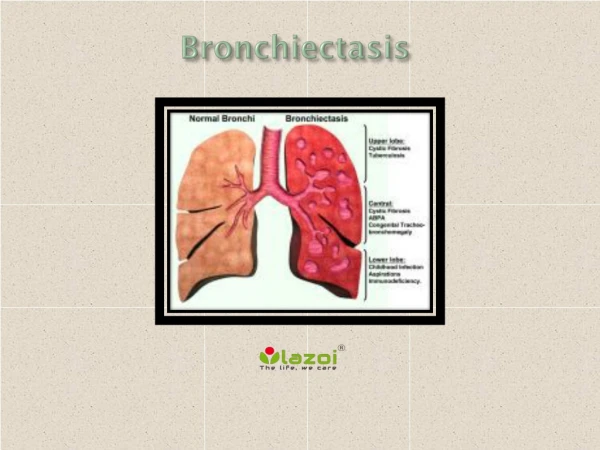
Current Therapies in Bronchiectasis. Dr Uğur Özçelik Hacettepe University, Department of Pediatric Pulmonology. Bronchiectasis is a condition characterized by the permanent dilation of bronchi with destruction of the elastic and muscular components of their walls.

E N D
Current Therapies in Bronchiectasis Dr Uğur Özçelik Hacettepe University, Department of Pediatric Pulmonology
Bronchiectasis is a condition characterized by the permanent dilation of bronchi with destruction of the elastic and muscular components of their walls
The goal of treatment of bronchiectasis • İmprove the symptoms of * cough *sputum production *dyspnea • Prevent the progression of airway damage
Treatment modalities of bronchiectasis • Non surgical/supportive Pharmacotherapy *Antibiotics *Bronchodilators *Mucolytics*Anti-inflammatory agents Chest physiotherapy • Surgery
New treatment options for bronchiectasis • Inhaled antibiotics • Hyperosmolar agents • Macrolides
Antibiotics at acute exacerbation • Acute exacerbations are clinically recognized by an increased sputum production that becomes purulent and thicker. • Acute excerbations are usually caused by the colonizing bacterial flora, and therapy should be directed towards these (H.influenzae, P.aeruginosa). • 10-14 days course of oral antibiotic will be sufficient in the majority of patients. • Parenteral administration should be reserved for those patients with severe impairment of lung function or acute respiratory failure, and those with chronic bronchial sepsis.
Prophylactic antibiotics in bronchiectasis • Prophylactic antibiotic use is considered for the patients who suffer frequent relapses; * necessiating oral antibiotic courses more than six times per year*hospital admissions for iv antibiotics more than two times a year.* rapid relapse within 1 month after iv antibiotic Expert opinion, lack of evidence based studiesExpert Opin Pharmacother 2007:8:3183
Inhaled antibiotics • Tobramycin • Colimycin ---------------------- • Aztreonam • Ciprofloxacin • Amikasin
Inhaled tobramycin • In patients with idiopathic bronchiectasis, although the treatment group had decreased density of P.aeruginosa and have an improvement in clinical findings they were also have adverse eventssuch as increased cough, dyspnea, wheezing and chest pain which causes of treatment intolerance. Am J Respir Crit Care Med 2000;162:481 Chest 2005;127:1420
Aim:To test the effect of adding inhaled tobramycin to oral ciprofloxacin. • Method: Double blind, randomized, parallel-design. 17 centers. U.K&USA. • 53 adults: P.aeruginosa + Acute exacerbation • Therapy: Cipro.+placebo/Cipro.+Tobra. • Parameters: Clinical symp., PFT, Clinical effic., Sputum microbiology. Chest 2006;130:1503.
Cipro.+Tobra;compared Cipro+Placebo; greater microbological response; but no statistically significant difference in clinical efficacy at days 14 or 21. Increased frequency of wheeze (%50 vs %15) Chest 2006;130:1503
Bronchodilators • Bronchodilators, including short acting and long acting β-agonists, anticholinergics can be used for bronchiectasis for bronchial hyperrreactivity or improve mucociliary clearance. • However, there have been no randomized studies that have validated their usefulness in the management of cough, sputum production, dyspnea in patients with bronchiectasis. • In patients with bronchiectasis with airflow obstruction and/or bronchial hyperreactivity, therapy with bronchodilators may be of benefit. Cochrane Database Syst Rev, 2004
Mucolytics • The purpose of mucolytic drugs is to assist tracheobronchial clearance by altering the properties of sputum.*N-acetly cystein*rh-DNase • There is little scientific evidence to recommend the routine use of mucolytic agents in bronchiectasis. Cochrane Database Syst Rev, 2004
Recombinant human DNase • DNA release by neutrophils in airways increases sputum viscosity, and rhDNase administered by aeresol digests DNA, thereby decreasing sputum viscosity, mucus plugging, infection and inflammation.
Aerosolized Recombinant Human DNase (Dornase Alfa) • Dornase alfa has been shown to improve lung function and decrease exacerbations, with regular administration to patients with CF. • A pilot study in bronchiectasis suggested that sputum viscosity and other clinical parameters were unchanged with dornase alfa.Am J Respir Crit Care Med 1996;154:413
Treatment of idiopathic bronchiectasis with aerosolized recombinant human DNase IChest 1998:113:1329. O’Donnell AE, et al. • 349 adult patients with bronchiectasis • Dornase alfa/placebo twice daily • 24 weeks Results • Dornase alfa group: more exacerbations more hospitalizations more antibiotic more steroid requierment Conclusion:Dornase alfa has no demonstrated efficacy in patients with idiopathic bronchiectasis.
Hyperosmolar agents • Hypertonic saline • Inhaled dry powder mannitol
Hypertonic saline • Two studies 7% saline solution in CF patients demonstrated benefits including improved PFT and a reduction of exacerbation • 24 BE patients, 4 days-4 different therapy (ACB,neb.terb+ACB, neb.terb+NS+ACB; neb.ter+7%HS+ACB).7%HS: produced more sputum, easiest sputum expectoration; small but significant differences in FEV1, FVC. NEJM 2006;354:229/241 Respir Med 2005;99:27
Inhaled dry powder mannitol • Inhalation of 400 mg of mannitol increased clearance of mucus acutely and 24 h in BE patients. • Mannitol improved the health-related quality of life in patients with BE when administered 2 wks. • A placebo controlled study, patients (185) received either 320 mg of mannitol, twice a day, or placebo (95) for 3 months. Results: better scores, lower antibiotic needs in mannitol group.Chest 2001;119:414;159:1843; ERJ 2004;Suppl 48:707;AJRCCM 2009;179:A3221
Anti-inflammatory agents • İnhaled corticosteroids • Macrolides
Inhaled corticosteroids • Two randomized short-time (4 and 6 weeks) placebo controlled trials of inhaled corticosteroids in patients with idiopathic bronhiectasis showed no effect on clinical findings (sputum production, cough, wheeze, or dyspnea) and nonsignificant improvement FEV1, FVC and CO diffusion.Respir Med 1992;86:121 Am J Respir Crit Care Med 1998;158:723)
Aim: to study the effects of inhaled steroid withdrawal on bronchial hyperreactivity, sputum inflammatory markers and neutrophilic apoptosis in non-CF bronchiectasis. • 27 BE children. • Metacholine challange; apoptotic neutrophil ratio, IL-8, TNF-alfa, neutrophil ratios in induced sputum, PFT before and after 12-week withdrawal of ICS. JClin Pharm Therapeutics 2008;33:603
Results: 12 week-withdrawal of ICS increased bronchial hyperreactivity, but no change in sputum inflammatory markers, decreased neutrophil apoptosis. JClin Pharm Therapeutics 2008;33:603
86 patients, 52 wks; placebo controlled, double blind, randomised study. 43 pt:500ug fluticazone; twice daily 43 pt:placebo Results: significantly more pt. on ICS than on placebo showed improvement in 24 h. sputum volume; but not exacerbation frequency FEV1, FVC, sputum purulence score.Better results in P.aeruginosa + pt.Thorax 2005;60:239
Macrolide therapy in bronchiectasis Antibacterial properties Immunmodulator properties • Decreasing mucus production • Inhibiting virulence factors and biofilm production of P. aeruginosa • Down regulation of inflammatory cytokines (TNF-alfa, IL-8, IL4, IL-1ß) and chemotaxis of neutropils • Activate ciliary movement • Decreasing leucocyte numbers • Acceleration of apoptosis of neutrophilsJ Infect Dis 1989;5:966; Antimicrobial Agents and Chemotherapy 1998;42:1605; ERJ 1999;13:1371; Pediatr Pulmonol 2001;31:464
Macrolide therapy in bronchiectasis • Five small clinical trials have assessed the effect of macrolides on bronchiectasis. • Reduced sputum volume • Improved lung function • Better symptom control • Side effects, resistance, drug interactions Eur Respir J 1999;13:361 J Clin Pharm Ther 2006:31:49 Respir Med 2008:102:1494
17 BE patients; randomized CAM or supportive treatment for 3 months.17 BE patients as control group. At initiation and at the end of 3 months. *BAL: IL-8, TNF-alfa, IL-10, cell profiles *PFT and sputum production measured. • Compared with the control group, the treatment group showed a significant decrease in IL-8 levels, total cell count, neutrophil ratios in BAL fluid and daily sputum production; increase BAL fluid macrophage ratios at the end of the third month • The differences in PFT were not significant. J Clin Pharmacy Therapeutics 2006;31:49-55
Chest physiotherapy In patients with conditions associated with the hypersecretion of mucus and the inability to expectorate effectively, chest physiotherapy should be used.
Surgery Two major indication of surgery • Patients with localized bronchiectasis if they suffer from frequent acute exacerbations despite appropriate medical management • Life-threatening infectious complications(lung abcesses) or massive haemopthysis that is not responding to medical treatment, or bronchial embolization
Surgery • Multisegmental or bilateral bronchiectasis is generally regarded as a contraindication for surgery. • Cases of bronchiectasis, with failure of conservative therapy, for which surgical intervention may be considered when the remaining lung is esentially unaffected.
Surgery • Some authors use hemodynamic (functional and morphologic) classification for the indication of surgery (HRCT and V/Q scan) • The area affected is considered indicated for surgery when the perfusion less than 10% of the expected at ventilation/perfusion lung scan. J Thorac Cardiovasc Surg 2005;130:1385)
Lung transplantation • Lung transplantation must be regarded as an alternative in end-stage lung disease, in patients with an expected survival of less than 2 years. • Of the 6126 lung transplant procedures recorded by the St. Louis International Lung Transplant Registry since January 1997, 932 patients had CF (15%) and 129 (2%) had non CF bronchiectasis. J. Heart Lung Transplant 1999; 18:611. • 1-year survival rate of 68% in bronchiectasis patients who underwent single and double lung transplants. J. Heart Lung Transplant 2005;24:1530.
Does knowing the etiology lead to changes in management? • The case records of all patients who were diagnosed as having bronchiectasis by CT (Royal Brompton Hospital, Great Ormond Street Hospital for Children, UK) • All patients had undergone extensive investigations for etiology. • 136 patients (median age 12.1; range 3.1-18.1). • Immunodeficiency, aspiration and PCD accounted for 67% of the cases.In 77 (56%) children, the identification of a cause led to a spesific change in management.Eur Respir J 2005;26:8
Conclusion Each patient with bronchiectasis must be evaluated individually for the etiology of bronchiectasis, severity of clinical findings, severity and extent of bronchiectasis and functions of the remaining lung tissue for the selection treatment modalities. Prospective, randomized, double-blind data are needed before new treatment options can be recommended as standart therapy.