Download
1 / 16
160 likes | 349 Views
Tissue Perfusion II Respiratory Pathophysiology. Paul Marshall. Pathophysiology: common mechanisms Inability to maintain normal blood gases Hypoxaemia Hypercapnia Possible mechanisms: IMPAIRED VENTILATION (hypoventilation) neuromuscular Motor neurone disease

E N D
Tissue Perfusion II Respiratory Pathophysiology Paul Marshall
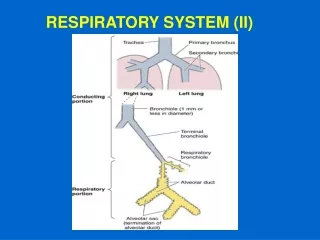
Pathophysiology: common mechanisms • Inability to maintain normal blood gases Hypoxaemia Hypercapnia • Possible mechanisms: IMPAIRED VENTILATION (hypoventilation) neuromuscular Motor neurone disease Brain stem damage (e.g CVA) obstruction COPD asthma bronchial tumour bronchiectasis
Possible mechanisms continued: IMPAIRED VENTILATION (cont:) alveolar damage emphysema fibrotic lung disease pleural damage pneumothorax IMPAIRED GASEOUS EXCHANGE pneumonia COPD pulmonary oedema ARDS IMPAIRED PERFUSION right to left shunts PE
Asthma: • acute reversible airway disease • due to increased reactivity of smooth muscle of bronchioles (inflammatory response) • may be episodic, chronic or severe acute • result: airway obstruction (bronchospasm and • oedema, excess sputum) - worse on • expiration • hypoventilation • hypoxaemia • retention of CO2
Asthma continued: clinical features • dyspnoea • expiratory wheeze and cough • anxiety/fear/restlessness • central cyanosis • low O2 sats < 90% • tachycardia • alteration in consciousness
Chronic Obstructive Pulmonary Disease (COPD) umbrella term which encompasses: emphysema chronic bronchitis chronic obstructive airways disease (COAD) characterised by: airways obstruction (variable reversibility) inflammatory/bronchitis component emphysema UK: 600,000 have COPD 26,000 die /year in England and Wales set to be fifth largest cause of death by 2020
Pathophysiology: • bronchitis/ inflammatory component: • major contributory factor is smoking • bronchial inflammation & oedema • mucous gland hypertrophy: • excess mucus production • impaired muco-ciliary clearance • increased bacterial growth in static • mucus • alveolar macrophages activated – • destroy alveolar wall • result: • decrease in FEV1 (CO2 retention) • hypoventilation (V/Q mismatch)
Emphysema component: • pathologically an increase in the size of air • spaces distal to terminal bronchioles with • destruction of alveolar walls • loss of lung elastic recoil • alveolar distension and rupture • compliance reduced • total lung capacity increases • residual volume increases • physiologic dead space increased • reduced diffusing capacity • Result: • hypoventilation(V/Q mismatch)
Emphysema – genetic factor: deficiency of 1-Antitrypsin (protein) 1-Antitrypsin protects against alevolar wall destruction by elastase deficiency allows unchecked destruction of alveolar wall
Overall pathophysiological effect: • airflow obstruction ( peak flow/FEV1) • hypoventilation • ventilation/perfusion (V/Q) mismatch • reduced diffusing capacity • CO2 retention (hypercapnia) • Hypoxaemia Reference: (Weinberger 1992, West 1992)
BTS guidelines (1997): FEV1 Drug choice (of predicted) MILD 80% short acting 2-agonist or inhaled anticholinergic MODERATE 60% short acting 2-agonist or inhaled anticholinergic or both (COMBIVENT) consider steroid trial SEVERE 40% consider combination therapy ? home nebuliser steroid trial ? other agents
Hypercapnia in COPD: additional mechanisms • fatigue of inspiratory muscles • alteration in breathing pattern ( Vt, Vf, dead space) • abnormalities of ventilatory drive: major stimulus is hypoxaemia complex mechanism may be reduced chemoreceptor responsiveness (Weinberger 1989, Lourenco & Miranda 1968)
Respiratory failure: • inability to maintain normal arterial PaO2 and • PaCO2 • two types: • Type I: PaO2 low (< 8.0 kPa) (hypoxaemia) • PaCO2 normal or low • (normal < 6.5 kPa) • Asthma • PE • Pulmonary oedema
Respiratory failure: continued Type II: PaO2 low (< 8.0 kPa) (hypoxaemia) PaCO2 raised (> 6.5 kPa) (hypercapnia) chronic bronchitis chest deformities respiratory centre depression e.g. opiates brain stem CVA
References: BTS (1997) British Thoracic Society guidelines: diagnosis & Management of COPD Thorax 52(suppl 5):S1-S32 Lourenco RV & Miranda JM (1968) Drive and performance of the Ventilatory apparatus in chronic obstructive lung disease NEJM 279:53-59 Weinberger SE et al (1989) Hypercapnia NEJM 321:1223-1231 Weinberger SE (1992) Principles of pulmonary medicine 2nd ed. WB Saunders Philadelphia West JB (1992) Pulmonary physiology- the essentials 4th ed. Williams & Wilkins Baltimore