Download
1 / 71
720 likes | 973 Views
Retroviruses. Groups of Retroviruses. Oncovirinae Tumor viruses and similar Lentiviruses Long latent period Progressive chronic disease Visna HIV Spumavirinae. important. important. Retroviruses known to cause human cancer. Human T cell lymphotropic virus -1 (HTLV-1)

E N D
Groups of Retroviruses • Oncovirinae • Tumor viruses and similar • Lentiviruses • Long latent period • Progressive chronic disease • Visna HIV • Spumavirinae important important
Retroviruses known to cause human cancer • Human T cell lymphotropic virus -1 (HTLV-1) • Adult T cell leukemia, Sezary T-cell leukemia • Africa, Caribbean, Some Japanese Islands • Human T cell lymphotropic virus -2 (HTLV-2) • Hairy cell leukemia • HIV?
HIV and AIDS • Acquired Immunodeficiency Syndrome • Disease caused by an infectious agent: • a retrovirus
With giemsa stain at high magnification, the faint bluish dot-like intracystic bodies of Pneumocystis carinii in lung are seen in this cytologic preparation from a bronchoalveolar lavage HIV and AIDSan infectious agent In Los Angeles1967-1978 only two cases of Pneumocystis carinii pneumonia All Homosexual • 1979 - 5 cases of Pneumocystis carinii
HIV and AIDS With dissemination to extrapulmonary sites, Pneumocystis carinii tends to produce foci with prominent calcification, as seen in the kidney here grossly.
HIV and AIDSan infectious agent – Kaposi’s Sarcoma • Early 1981 MMWR: 5 cases of Kaposi’s sarcoma • Hitherto: rare (immunocompromization) • 1981 - 26 cases of Kaposi’s sarcoma • Young • San Francisco and New York • All Homosexuals
HIV and AIDS Two rare diseases in the gay community linked to IMMUNOSUPPRESSION OPPORTUNISTIC INFECTIONS Also Lymphadenopathy Hodgkin’s Lymphoma • Gay-Related Immune Deficiency • Acquired Immune Deficiency Syndrome (AIDS)
HIV and AIDS Distinguishing characteristics • Clusters of infected men • Apparent concentration within sexually interactive groups • High numbers of sex partners Suggests an infectious agent
HIV and AIDS • More evidence for an infectious agent: • Different ways of getting a similar syndrome • Blood transfusions • Intravenous drug use • Hemophilia (clotting factor) Female sex partners of AIDS-positive IV drug users and hemophiliacs Not just in the Gay community
HIV and AIDS Obvious agent: A virus……that is now in the blood supply Primary route of transmission: Sex AIDS is a sexually-transmitted disease
HIV and AIDS The Cellular Picture Loss of one cell type throughout the course of the disease CD4+ T4 helper cells A fall in the CD4+ cells always precedes disease In advanced disease the loss of another cell type CD8+ cytotoxic killer cells Suggests an infectious agent A virus
AIDS Definition • AIDS is currently defined in persons older than 13 years as the presence of one of 25 conditions indicative of severe immunosuppression or • HIV infection in an individual with a CD4+ cell count of <200 cells per cubic mm of blood. • AIDS is therefore the end point of an infection that is continuous, progressive and pathogenic • With the prevalence of HIV in the developing world, HIV and its complications will be with us for generations
HIV and AIDSThe Virus • The virus only grows on T4 cells that are proliferating in response to an immune stimulus • Therefore difficult to grow in culture • Robert Gallo : reverse transcriptase in activated T4 cells in blood of patients with AIDS : HTLV-3 • Luc Montagnier: LAV • Human Immunodeficiency Virus (HIV)
GENOSOME • Diploid Capped and polyadenylated • Positive sense (same as mRNA) Viral RNA cannot be read as mRNA New mRNA must be made Virus must make negative sense DNA before proteins are made Therefore virus must carry REVERSE TRANSCRIPTASE into the cell
The Genome of HIV • Three structural genes • LTRs • Extra open reading frames are clue to latency • These ORFs code for small proteins - antibodies in AIDS patients
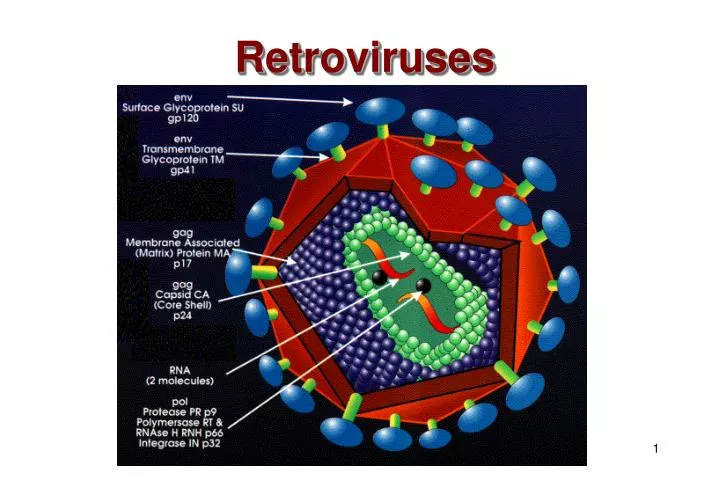
A HIV has: 3 structure genes GAG : internal proteins ENV: Envelope glycoproteins • POL: Enzymes • Reverse transcriptase • Integrase • Protease (cuts polyproteins)
Membrane: host derived Two glycoproteins: gp160 gp120 and gp41 gp41 is fusogen that spans the membrane sugars: immunosilent HIV - The Virus vaccine problem
p17: inner surface p24: nucleocapsid p9: nucleocapsid associated with RNA HIV - The Virus Group-Specific Antigens GAG gene
The Genome of HIV Small non-structural proteins mRNAs made by multiple splicing of genomic RNA (c.f. mRNA for structural proteins) • EARLY • TAT: TransActivator of Transcription • REV: Regulator of Virion Protein Expression • NEF: Negative Regulatory Factor • LATE • VIF: Virion Infectivity Factor • VPU: Viral Protein U • VPR: Viral Protein R TAT and REV are essential for HIV replication
HIV - Life History • A retrovirus • Latency • Specific destruction of CD4+ cells • How does the virus enter the cell?
HIV - Life History Entry into the cell T4 (CD4+) cells are major target Human HeLa Cell transfected with CD4 antigen Human HeLa Cell NOT INFECTED INFECTED But NOT the whole answer since this does not happen if CD4 is transfected into a MOUSE cell
HIV - Life History • Fusion at ambient pH • No need for entry into lysosomes • Syncytia Profound significance for AIDS progression Profound significance for therapy
Co-Receptors CD8+ Cells MIP-1 alpha MIP-1 beta RANTES Chemokines Block HIV infection of macrophages HIV - Life History Why do CD4-transfected human cells become infected but CD4-transfected mouse cells do not? Human cells must possess a co-factor for infection that mouse cells do not
HIV - Life History HIV chemokine Mutant CCR5 CD4 CCR5 CD4 CCR5 CD4 macrophage
HIV and AIDS Co-receptors CCR5 is a chemokine receptor 25% of long term survivors are CCR5 or CCR2 mutants (deletions) Many other chemokine receptors
Endocytosis Fusion of membranes Release of nucleocapsid to cytoplasm Nucleus HIV – life history
HIV - Life History HIV carries with it: • Reverse transcriptase • Integrase • Protease • tRNA primer HIV genes GAG POL ENV HIV has no oncogene but could still be oncogenic vaccine problem
virus virus HIV – life history RNA-dependent DNA Polymerase encoded by virus REVERSE TRANSCRIPTASE RNA genome Reverse transcriptase DNA genome Integrase Integrates Host RNA polymerase II RNA genome host
HIV – life history • Parental RNA • RNA/DNA Hybrid • Linear DNA/DNA duplex • Circular Duplex DNA • Integration Replication (DNA genome in cell) • Transcription Viral RNA genome mRNA protein Reverse transcriptase Reverse transcriptase Integrase Host DNA polymerase Host splicing enzymes Host RNA pol II
LIFE HISTORY OF HIV
HIV - Life History Latency - Cellular Only activated T4 cells can replicate virus Most infected T4 cells are rapidly lyzed but are replaced Some T4 cells revert to resting state as memory cells which are long-lived Memory T4 cells cannot replicate the virus unless the become activated Macrophages do not show latency Clinical Latency HIV infection is not manifested as disease for years During apparent clinical latency, virus is being replicated and cleared
Chronically-infected memory T cells with provirus Return to resting state Infection Long lived! Reactivation Long lived! Uninfected unactivated memoryT cell pool Dynamics of CD4 T cells in an HIV infection Cell deathapoptosis etc Uninfected activated T cell Cell deathimmunedestruction Adapted from Saag and Kilby Nat Med 5: 609, 1999
Latency In the absence of any activating stimulus: Homeostasis
Immune response T4 activated HIV production Latency Breaks T4 resting
The cellular and immunological picture - The course of the disease HIV and AIDS
The cellular and immunological picture - The course of the disease HIV and AIDS
HIV and AIDS The cellular and immunological picture The course of the disease 1. Acute Infection • High virus titer • Mild symptoms • Fall in CD4+ cells but recovers • Rise in CD8+ cells but recovers • A high virus titer (up to 10 million viruses per ml blood) • Macrophages infected Macrophages bring HIV into the body if sexually transmitted
HIV and AIDS 2. A strong immune response • Virus almost disappears from circulation • Good cytoxic T cell response • Soluble antibodies appear later against both surface and internal proteins • Most virus at this stage comes from recently activated (dividing) and infected CD4+ cells • CD4+ cell production compensates for loss due to lysis of cells by virus production and destruction of infected cells by CTLs
HIV and AIDS 3. A latent state • Latency of virus and of symptoms • Virus persists in extra-vascular tissues • Lymph node dendritic cells • Resting CD4+ memory cells (last a very long time - a very stable population of cells) carry provirus
HIV and AIDS • 10 billion HIV particles per day • Virus half life 5.7 hours • 100-10 million virions per ml blood (set point) • Small minority of T4 cells are infected • Virus found in lymph nodes
HIV and AIDS 4. The beginning of disease • Massive loss of CD4+ cells • CD4+ cells are the targets of the virus • Cells that proliferate to respond to the virus are killed by it: Clonal deletion • Dendritic cells present antigen and virus to CD4 cells just as they are activated • Epitope variation allows more and more HIV to escape from immune response just as response wanes • Apoptosis of CD4+ cells • HIV patients with high T4 cell counts do not develop AIDS
HIV and AIDS 5. Advanced disease - AIDS • CD8+ cells destroy more CD4+ cells • CD4 cell loss means virus and infected cells no longer controlled • As CD4+ cells fall below 200 per cu mm virus titer rises rapidly and remaining immune response collapses • CD8+ cell number collapses • Opportunistic infections • Death in ~2 years without intervention
Inexorable decline of CD4+ T4 cells Why do all of the T4 cells disappear? At early stages of infection only 1 in 10,000 cells is infectedLate 1 in 40 Of great importance to therapeutic strategy
Virus destroys the cell as a result of budding But few cells are infected: Early stage of infection 1:10,000 Late 1:40 HIV could kill sub population of precursor cells People develop AIDS even when they have HIV that does not lyze cells Why do all T4 cells disappear? 1. PUNCTURED MEMBRANE