Download
1 / 69
710 likes | 739 Views
Genetic Variation in Individuals and Populations: Mutation and Polymorphism. FACTORS THAT DISTURB HARDY-WEINBERG EQUILIBRIUM.

E N D
Genetic Variation in Individuals and Populations: Mutation and Polymorphism
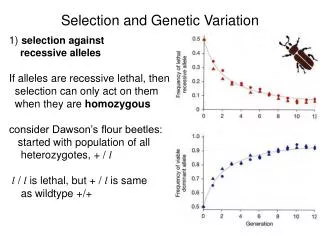
FACTORS THAT DISTURB HARDY-WEINBERG EQUILIBRIUM • A number of assumptions underlie the Hardy-Weinberg law. First is that the population is large and mating is random. A very small population in which random events can radically alter an allele frequency may not meet this first assumption. • This first assumption is also breached when the population contains subgroups whose members choose to marry within their own subgroup rather than the population at large. • Second is that allele frequencies are not changing over time. This means that there is no migration in or out of the population by groups whose allele frequencies at a locus of interest are radically different from the allele frequencies in the population as a whole.
Similarly, selection for or against particular alleles and new mutations adding alleles to the gene pool break the assumptions of the Hardy-Weinberg law. • In practice, some of these violations are more damaging than others to the application of the law to human populations. Violating the assumption of random mating can cause large deviations from the frequency of individuals homozygous for an autosomal recessive condition that we might expect from population allele frequencies.
On the other hand, changes in allele frequency due to mutation, selection, or migration usually cause more minor and subtle deviations from Hardy-Weinberg equilibrium. • Finally, when Hardy-Weinberg equilibrium does not hold for a particular disease allele at a particular locus, it may be instructive to investigate why the allele and its associated genotypes are not in equilibrium.
Exception to Large Population with Random Mating • The principle of random mating is that for any locus, an individual of a given genotype has a purely random probability of mating with an individual of any other genotype, the proportions being determined only by the relative frequencies of the different genotypes in the population. • One's choice of mate, however, may not be at random. In human populations, nonrandom mating may occur because of three distinct but related phenomena: stratification, assortative mating, and consanguinity.
Stratification • Stratification describes a population in which there are a number of subgroups that have remained relatively genetically separate during modern times. • Worldwide, there are numerous stratified populations; for example, the U.S. population is stratified into many subgroups including whites, African Americans, and numerous Native American, Asian, and Hispanic groups.
Similarly stratified populations exist in other parts of the world as well. When mate selection in a population is restricted to members of one particular subgroup within that population, the result for any locus with more than one allele is an excess of homozygotes in the population as a whole and a corresponding deficiency of heterozygotes compared with what one would predict under random mating from allele frequencies in the population as a whole.
Suppose a population contains a minority group constituting 10% of the population in which a mutant allele for an autosomal recessive disease has a frequency qmin = 0.05. • In the remaining majority 90% of the population, qmaj is 0. An example of just such a situation is the African American population of the US and the mutant allele at the β-globin locus responsible for sickle cell disease. • The overall frequency of the disease allele in the total population, qpop, is therefore equal to 0.05/10 = 0.005, and, simply applying the Hardy-Weinberg law, the frequency of the disease in the population as a whole would be q2pop = 0.000025 if mating were perfectly random throughout the entire population.
If, however, a minority group mates nearly exclusively with other members of the minority group, then the frequency of affected individuals in the minority group would be (q2min) = 0.0025. • Because the minority group is one tenth of the entire population, the true frequency of disease in the total population is 0.0025/10 = 0.00025, 10-fold higher than one would expect from applying the Hardy-Weinberg law to the population as a whole without consideration of stratification. • By way of comparison, stratification has no effect on the frequency of autosomal dominant disease and would have only a minor effect on the frequency of X-linked disease by increasing the small number of females homozygous for the mutant allele.
Assortative Mating • Assortative mating is the choice of a mate because the mate possesses some particular trait. • Assortative mating is usually positive; that is, people tend to choose mates who resemble themselves (e.g., in native language, intelligence, stature, skin color, etc.) • To the extent that the characteristic shared by the partners is genetically determined, the overall genetic effect of positive assortative mating is an increase in the proportion of the homozygous genotypes at the expense of the heterozygous genotype.
A clinically important aspect of assortative mating is the tendency to choose partners with similar medical problems, such as congenital deafness or blindness or exceptionally short stature (dwarfism). • In such a case, the expectations of Hardy-Weinberg equilibrium do not apply because the genotype of the mate at the disease locus is not determined by the allele frequencies found in the general population. • For example, in the case of two parents with achondroplasia, offspring homozygous for the achondroplasia gene have a severe, lethal form of dwarfism that is almost never seen unless both parents are achondroplasia heterozygotes.
When mates have autosomal recessive disorders caused by the same mutation or by allelic mutations in the same gene, all of their offspring will also have the disease. • Of course, not all blindness, deafness, or short stature has the same genetic basis; many families have been described, for example, in which two parents with albinism have had children with normal pigmentation or two deaf parents have had hearing children because of locus heterogeneity.
Even if there is genetic heterogeneity with assortative mating, however, the chance that two individuals are carrying mutations in the same disease locus is increased over what it would be under true random mating, and therefore the risk of the disorder in their offspring is also increased. • Although the long-term population effect of this kind of positive assortative mating on disease gene frequencies is insignificant, a specific family may find itself at very high genetic risk.
Consanguinity and Inbreeding • Consanguinity, like stratification and positive assortative mating, brings about an increase in the frequency of autosomal recessive disease by increasing the frequency with which carriers of an autosomal recessive disorder mate. • Unlike the disorders in stratified populations, in which each subgroup is likely to have a high frequency of a few alleles, the kinds of recessive disorders seen in the offspring of related parents may be very rare and unusual because consanguineous mating allows uncommon alleles to become homozygous.
Similarly, in genetic isolates, the chance of mating with another carrier of a particular recessive condition may be as high as that observed in cousin marriages, a phenomenon known as inbreeding. • For example, among Ashkenazi Jews in North America, mutant alleles for Tay-Sachs disease (GM2 gangliosidosis) are relatively more common than in other ethnic groups. • The frequency of Tay-Sachs disease is 100 times higher in Ashkenazi Jews (1 in 3600) than in most other populations (1 in 360,000). Thus, the Tay-Sachs carrier frequency among Ashkenazi Jews is approximately one in 30 (q2 = 1/3600, q = 1/60, 2pq = ~1/30) as compared to a carrier frequency of about one in 300 in non-Ashkenazis.
Exceptions to Constant Allele Frequencies Genetic Drift in Small Populations • Chance events can have a much greater effect on allele frequencies in a small population than in a large one. If the population is small, random effects, such as increased fertility or survival of the carriers of a mutation, occurring for reasons unrelated to carrying the mutant allele (which would be selection, not a random event), may cause the allele frequency to change from one generation to the next.
In a large population, such random effects would average out, but in a small population, allele frequencies can fluctuate from generation to generation by chance. • This phenomenon, known as genetic drift, can explain how allele frequencies can change as a result of chance operating on the small gene pool contained within a small population.
Mutation and Selection • In contrast to nonrandom mating, which can substantially upset the relative frequency of various genotypes predicted by Hardy-Weinberg equilibrium, changes in allele frequency due to selection or mutation usually occur slowly, in small increments, and cause much less deviation from Hardy-Weinberg equilibrium, at least for recessive diseases. • Mutation rates are generally well below the frequency of heterozygotes for autosomal recessive diseases, and so new mutation would have little effect in the short term on allele frequencies for such diseases.
In addition, most deleterious recessive alleles are hidden in heterozygotes and not subject to selection. As a consequence, selection is not likely to have major short-term effects on the allele frequency of these recessive alleles. • Therefore, to a first approximation, Hardy-Weinberg equilibrium may apply even for alleles that cause severe autosomal recessive disease. • For dominant or X-linked disease, however, mutation and selection do perturb allele frequencies from what would be expected under Hardy-Weinberg equilibrium by substantially reducing or increasing certain genotypes.
Fitness is the chief factor that determines whether a mutation is lost immediately, becomes stable in the population, or even becomes, over time, the predominant allele at the locus concerned. • The frequency of an allele in a population represents a balance between the rate at which mutant alleles appear through mutation and the effects of selection. • If either the mutation rate or the effectiveness of selection is altered, the allele frequency is expected to change.
Whether an allele is transmitted to the succeeding generation depends on its fitness (f), which is a measure of the number of offspring of affected persons who survive to reproductive age, compared with an appropriate control group. • If a mutant allele is just as likely as the normal allele to be represented in the next generation, f equals 1. If an allele causes death or sterility, selection acts against it completely, and f equals 0. • A related parameter is the coefficient of selection,s, which is a measure of the loss of fitness and is defined as 1 - f, that is, the proportion of mutant alleles that are not passed on and are therefore lost as a result of selection.
In the genetic sense, a mutation that prevents reproduction by an adult is just as lethal as one that causes a very early miscarriage of an embryo, because in neither case is the mutation transmitted to the next generation. • Fitness is thus the outcome of the joint effects of survival and fertility. In the biological sense, fitness has no connotation of superior endowment except in a single respect: comparative ability to contribute to the gene pool of the next generation.
Selection in Recessive Disease • Selection against harmful recessive mutations has far less effect on the population frequency of the mutant allele than does selection against dominant mutations because only a small proportion of the genes are present in homozygotes and are therefore exposed to selective forces. • Even if there were complete selection against homozygotes (f = 0), as in many lethal autosomal recessive conditions, it would take many generations to reduce the gene frequencyappreciably because most of the mutant alleles are carried by heterozygotes with normal fitness.
For example, the frequency of mutant alleles causing phenylketonuriaq, is approximately 1% in many white populations. Two percent of the population (2 × p × q) is heterozygous, with one mutant allele, whereas only 1 individual in 10,000 (q2) is a homozygote with two mutant alleles. The proportion of mutant alleles in homozygotes is given by:
Thus, only approximately 1% of all the mutant alleles in the population are in affected homozygotes and therefore are exposed to selection if dietary treatment were not available. • Removal of selection against an autosomal recessive disorder such as PKU by successful medical treatment would have just as slow an effect on increasing the gene frequency over many generations. • Thus, as long as mating is random, genotypes in autosomal recessive diseases can be considered to be in Hardy-Weinberg equilibrium, despite selection against homozygotes for the recessive allele. • The mathematical relationship between genotype and allele frequencies described in the Hardy-Weinberg law holds for most practical purposes in recessive disease.
Selection in Dominant Disorders • Dominant mutant alleles are directly exposed to selection, in contrast to recessive mutant alleles, most of which are "hidden" in heterozygotes. • Consequently, the effects of selection and mutation are more obvious and can be more readily measured for dominant traits. • A genetic lethal dominant allele, if fully penetrant, is exposed to selection in heterozygotes, removing all alleles responsible for the disorder in a single generation. • Several human diseases are thought or known to be autosomal dominant traits with zero or near-zero fitness and thus always result from new rather than inherited autosomal dominant mutations (Table 9-9).
Table 9-9. Examples of Disorders Occurring as Sporadic Conditions due to New Mutations with Zero Fitness
In some, the genes and specific mutant alleles are known, and family studies show new mutations in the affected individuals that were not inherited from the parents. • In other conditions, the genes are not known, but a paternal age effect has been seen, suggesting (but not proving) a new mutation in the paternal germline as a possible cause of the disorder. • The implication for genetic counseling is that the parents of a child with an autosomal dominant, genetic lethal condition have a low risk of recurrence because the condition would generally require another independent mutation to recur (except that the possibility of germline mosaicism must be kept in mind).
Mutation and Selection Balance in Dominant Disease • If a dominant disease is deleterious but not lethal, affected persons may reproduce but will nevertheless contribute fewer than the average number of offspring to the next generation; that is, their fitness, f, may be reduced. • Such a mutation is lost through selection at a rate proportional to the loss of fitness of heterozygotes. • The frequency of the mutant alleles responsible for the disease in the population therefore represents a balance between loss of mutant alleles through the effects of selection and gain of mutant alleles through recurrent mutation.
A stable allele frequency is reached at whatever level balances the two opposing forces: one (selection) that removes mutant alleles from the gene pool and one (new mutation) that adds new ones back. The mutation rate per generation, μ, at a disease locus must be sufficient to account for that fraction of all the mutant alleles (allele frequency q) that are lost by selection from each generation. Thus, μ = sq
When a genetic disorder limits reproduction so severely that the fitness is zero (s = 1), it is referred to as a genetic lethal. • For a dominant genetic lethal disorder, every allele in the population must be a new mutation since none can be inherited (in the absence of gonadal mosaicism). • In achondroplasia, the fitness of affected patients is not zero, but they have only about one fifth as many children as people of normal stature in the population. Thus, their average fitness, f, is 0.20, and the coefficient of selection, s, is 0.80. • In the subsequent generation, only 20% of current achondroplasia alleles are passed on from the current generation to the next. Because the frequency of achondroplasia is not decreasing, new mutations must be responsible for replacing the 80% of mutant genes in the population lost through selection.
If the fitness of affected persons suddenly improved (because of medical advances, for example), the observed incidence of the disease in the population would increase and reach a new equilibrium. • Retinoblastoma and certain other dominant embryonic tumors with childhood onset are examples of conditions that now have a greatly improved prognosis, with a predicted consequence of increased disease frequency in the population. • Allele frequency, mutation rate, and fitness are related; thus, if any two of these three characteristics are known, the third can be estimated.
Mutation and Selection Balance in X-Linked Recessive Mutations • For those X-linked phenotypes of medical interest that are recessive, or nearly so, selection occurs in hemizygous males and not in heterozygous females, except for the small proportion of females who are manifesting heterozygotes with low fitness. • Because males have one X chromosome and females two, the pool of X-linked alleles in the entire population's gene pool will be partitioned, with one third of mutant alleles present in males and two thirds in females.
As we saw in the case of autosomal dominant mutations, mutant alleles lost through selection must be replaced by recurrent new mutations to maintain the observed disease incidence. • If the incidence of a serious X-linked disease is not changing and selection is operating against, and only against, hemizygous males, the mutation rate, μ, must equal the coefficient of selection, s (the proportion of mutant alleles that are not passed on), times q, the allele frequency, times 1/3 since selection is operating on only one third of the mutant alleles in the population, that is, those present in males. Thus, μ = sq / 3
For an X-linked genetic lethal disease, s = 1 and one third of all copies of the mutant gene responsible is lost from each generation. • Therefore, one third of all persons who have such X-linked lethal disorders are predicted to carry a new mutation, and their genetically normal mothers have a low risk of having subsequent children with the same disorder (assuming no mosaicism). • In less severe disorders such as hemophilia A, the proportion of affected individuals representing new mutations is less than one third (currently about 15%).
Because the treatment of hemophilia is improving rapidly, the total frequency of mutant alleles can be expected to rise relatively rapidly and to reach a new equilibrium, as we saw in the case of autosomal dominant conditions. • Assuming that the mutation rate at this locus stays the same, the proportion of hemophiliacs who result from a new mutation will decrease, even though the incidence of the disease increases. Such a change would have significant implications for genetic counseling for this disorder.
Migration and Gene Flow • Migration can change allele frequency by the process of gene flow, defined as the slow diffusion of genes across a barrier. • Gene flow usually involves a large population and a gradual change in gene frequencies. • The genes of migrant populations with their own characteristic allele frequencies are gradually merged into the gene pool of the population into which they have migrated. (The term migrant is used here in the broad sense of crossing a reproductive barrier, which may be racial, ethnic, or cultural and not necessarily geographical and requiring physical movement from one region to another.)
The frequencies of the 32-base pair deletion allele of the CCR5 cytokine receptor gene, ΔCCR5, have been studied in many populations all over the world. • The frequency of the ΔCCR5 allele is highest, approximately 10%, in western Europe and Russia and declines to a few percent in the Middle East and the Indian subcontinent. • The ΔCCR5 allele is virtually absent from Africa and the Far East, suggesting that the mutation originated in whites and diffused into the more easterly populations.
Figure 9-10 Frequency of ΔCCR5 alleles in populations from Europe, the Middle East, and the Indian subcontinent.
Another example of gene flow between population groups is reflected in the frequency of specific mutant alleles causing PKU. • There is strong evidence that the most common mutations were of Celtic origin. These same mutations have now turned up in many populations around the world. • The presence of the same PKU alleles in different populations reflects the geographical migration of the Celts. • Thus, the frequency of PKU is approximately 1/4500 in Ireland, but the disorder is progressively less prevalent across northern and southern Europe. • There has been considerably less gene flow to East Asia; the incidence of PKU in Japan is only about 1/109,000.
ETHNIC DIFFERENCES IN THE FREQUENCY OF VARIOUS GENETIC DISEASES • The previous discussion of the Hardy-Weinberg law explained how, at equilibrium, genotype frequencies are determined by allele frequencies and remain stable from generation to generation, assuming the allele frequencies in a large, isolated, randomly mating population remain constant. • However, there is a problem of interest to human geneticists that the Hardy-Weinberg law does not address: Why are allele frequencies different in different populations in the first place? In particular, why are some mutant alleles that are clearly deleterious when present in homozygotes relatively common in certain population groups and not in others?
The human species of more than 6 billion members is separated into many subpopulations, or ethnic groups, distinguishable by appearance, geographical origin, and history. • Although the 25,000 genes and their location and order on the chromosomes are nearly identical in all humans, we saw earlier that extensive polymorphism exists between individuals in a population. • Most variation is found in all human populations, at similar frequencies. Other alleles, however, although present in all groups, may demonstrate dramatic differences in frequency among population groups; and finally, some allelic variants are restricted to certain populations, although they are not necessarily present in all members of that group.
It is likely that because modern humans lived in small isolated settlements until quite recently, as mutations occurred in the various groups, the differences in the frequency of certain alleles persisted and could even become magnified. • A number of factors are thought to allow differences in alleles and allele frequencies among ethnic groups to develop. • Two such factors are genetic drift, including nonrandom distribution of alleles among the individuals who founded particular subpopulations (founder effect), and heterozygote advantage under environmental conditions that favor the reproductive fitness of carriers of deleterious mutations.
For the population geneticist and anthropologist, selectively neutral genetic markers provide a means of tracing human history by tracking gene flows. • For example, some polymorphisms exist only in populations in sub-Saharan Africa, resulting in more polymorphic diversity among sub-Saharan Africans themselves than there is between sub-Saharan Africans and any other ethnic groups. • These data support the notion that modern humans in Africa developed substantial genetic diversity over a million years or more, well before the rest of the world's populations were derived 40,000 to 100,000 years ago from smaller subgroups that migrated out of Africa, carrying a more limited genetic diversity.
Differences in frequencies of alleles that cause genetic disease are significant for the medical geneticist and genetic counselor because they cause different disease risks in specific population groups. • Well-known examples include Tay-Sachs disease in people of Ashkenazi Jewish ancestry, sickle cell disease in African Americans, and cystic fibrosis and PKU in white populations. • The inherited disease of hemoglobin, β-thalassemia, is a clear example of ethnic differences both in disease frequency and in which alleles are responsible in populations with a high incidence of disease.
The disease is common in people of Mediterranean or East Asian descent and very rare in other ethnic groups. Even though dozens of different alleles can cause β-thalassemia, certain alleles tend to be far more common in some populations than in others, so that each population has only a few common alleles. • For example, the most common β-thalassemia alleles responsible for more than 90% of the disease in Mediterranean people are very rare in people from Southeast Asia or the Asian subcontinent; similarly, the most common alleles in Southeast Asians and Asian Indians are quite rare in the other two unrelated ethnic groups.
This information is of value in genetic counseling and prenatal diagnosis. For example, in North America, when persons of Mediterranean descent are at risk of having a child with β-thalassemia, testing of parental DNA for just seven mutant alleles has a more than 90% probability of providing the information needed for prenatal diagnosis
Table 9-10. Incidence, Gene Frequency, and Heterozygote Frequency for Selected Autosomal Disorders in Different Populations
Table 9-10. Incidence, Gene Frequency, and Heterozygote Frequency for Selected Autosomal Disorders in Different Populations
Genetic Drift • Genetic drift can explain a high frequency of a deleterious disease allele in a population. For example, when a new mutation occurs in a small population, its frequency is represented by only one copy among all the copies of that gene in the population. • Random effects of environment or other chance occurrences that are independent of the genotype and operating in a small population can produce significant changes in the frequency of the disease allele. • During the next few generations, although the population size of the new group remains small, there may be considerable fluctuation in gene frequency. These changes are likely to smooth out as the population increases in size. • In contrast to gene flow, in which allele frequencies change because of admixture, the mechanism of genetic drift is chance.