Download
1 / 76
811 likes | 1.16k Views
Acute adverse reactions to transfusion: a symptoms-based approach. Kathryn E. Webert, MD, MSc, FRCPC Assistant Professor, Departments of Medicine and Molecular Medicine and Pathology McMaster University, Hamilton, Ontario Associate Medical Director, Canadian Blood Services, Hamilton Centre.

E N D
Acute adverse reactions to transfusion: a symptoms-based approach Kathryn E. Webert, MD, MSc, FRCPC Assistant Professor, Departments of Medicine and Molecular Medicine and Pathology McMaster University, Hamilton, Ontario Associate Medical Director, Canadian Blood Services, Hamilton Centre
Summary of presentation • What is a transfusion reaction ? • Classification of transfusion reactions • Approach to acute transfusion reactions based on common presenting symptom: • Fever • Dyspnea • Rash/allergic symptoms **Detailed pathophysiology, management, and prevention was covered for most of these reactions in recent presentation**
What is a transfusion reaction? • Any untoward event that occurs as a result of infusion of a blood component (immediate or delayed) • When any unexpected or untoward sign or symptom occurs during or shortly after the transfusion of a blood component, a transfusion reaction must be considered as the precipitating event until proven otherwise • Only a high index of suspicion will allow a transfusion reaction to be diagnosed
Acute hemolytic transfusion reaction Febrile non-hemolytic transfusion reaction Allergic reactions Urticarial Anaphylactic Transfusion-associated circulatory overload (TACO) Transfusion-associated dyspnea (TAD) Transfusion-related acute lung injury (TRALI) Septic transfusion reaction (bacterial contamination) Hypotensive reactions ACE Inhibitors Non-immune red cell hemolysis Metabolic disturbances Hypothermia Hyperkalemia Acidosis Immediate Adverse Effects Associated with Transfusion
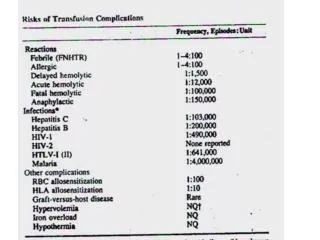
Immediate Adverse Effects Associated with Transfusion: risks
Delayed Adverse Effects Associated with Transfusion • Delayed hemolytic transfusion reaction • Alloimmunization • Red Cell Antigens • HLA • Leukocytes • Platelets • Graft versus host disease (TA-GVHD) • Post-transfusion purpura (PTP) • Hemosiderosis • Viral and parasitic infections • Transfusion-related immunomodulation (TRIM)
Signs and Symptoms of TR • Fever/chills/rigors • Pain • Dyspnea/respiratory distress • Bleeding • Hypotension • Hypertension • Headache • Nausea and vomiting • Rash/Hives • Angioedema • Anaphylaxis • Cyanosis • Bronchospasm • Tachycardia • Abdominal cramps • Diarrhea • Cough • Red eye • Anxiety • Jaundice
Classification of reaction by predominant symptom/sign • This presentation will focus on 3 common presenting symptoms and signs: • Fever • Dyspnea • Rash and other allergic reaction
Disclaimer: This is not easy… • Sometimes the patient has not read the text book… • More than one predominant presenting symptom • More than one reaction going on • Atypical presentation • Underlying comorbidities unrelated to transfusion
Approach to Patient with a Transfusion Reaction • 65 year old man develops shortness of breath and hypoxia while receiving unit of PRBC. • What is the differential diagnosis?
Approach to acute transfusion reactions commonly presenting with shortness of breath
Differential Diagnosis of TR with SOB • Transfusion-related acute lung injury (TRALI) • Circulatory overload (TACO) • Transfusion associated dyspnea (TAD) • Anaphylaxis • Acute hemolytic transfusion reaction • Bacterial contamination • Other etiology unrelated to transfusion SOB is usually the predominant symptom
Differential Diagnosis of TR with SOB: Background • Transfusion-related acute lung injury (TRALI) • Circulatory overload (TACO) • Transfusion associated dyspnea (TAD) • Anaphylaxis • Acute hemolytic transfusion reaction • Bacterial contamination • Other etiology unrelated to transfusion
Canadian Consensus Conference Definition of TRALI • During or within 6 hrs of transfusion • Acute lung injury • Acute onset • Hypoxemia • PaO2/FIO2 300 • SpO2 < 90% on room air • Bilateral infiltrates on CXR • No evidence of circulatory overload (PCWP18) • No preexisting ALI or other RF for ALI Kleinman et al. Transfusion 2004;44:1774-89 Toy et al. Crit Care Med 2005;33:721-6
TRALI: symptoms and signs • Virtually all patients have: • Shortness of breath • Hypoxia • Bilateral lung infitrates on CXR • May also have: • Hypotension • Fever • Transient leukopenia • Other: • Chest findings on auscultation tend to be minimal • No evidence of circulatory overload Bux and Sachs. Transfusion Medicine and Hemotherapy. 2008
TRALI: Epidemiology • 0.4 to 1.6 cases per 1,000 patients transfused • Likely under-reported and under-recognized • Described with all blood products • Usually contain > 60 mL plasma • US FDA observed TRALI to be the leading cause of transfusion related deaths 2003-2008. • Responsible for 16 to 65% of transfusion-related mortalities • In Canadian TTISS Report (2004-2005): • 2nd highest cause of transfusion-related morbidity and mortality Fatalities reported to FDA following blood collection and transfusion. Annual Summary for Fiscal Year 2008. Transfusion Transmitted Injuries Surveillance System, Program Report 2004-2005, Public Health Agency of Canada, March 2008
Donor alloantibody TRALI: Pathophysiology Immune • Passive transfer of donor alloantibodies in plasma of transfused product • Anti-HLA (Class I) • Anti-HLA (Class II) • Human neutrophil antigens (HNA) • Antibody binding to circulating WBC (and perhaps also pulmonary endothelium) causes cellular activation Recipient WBC
TRALI: Pathophysiology Non-immune • TRALI is also caused by the infusion of “biologic response modifiers” within the blood component • Cytokines (IL-6, IL-8, IL-1, TNF-a) • Lipids with neutrophil-priming activity • CD40 ligand • These substances accumulate in cellular blood products with prolonged storage Silliman CC et al., Transfusion 1997 Silliman CC et al., Blood 2003
TRALI: Diagnosis • No test with which to diagnose TRALI. • TRALI should be suspected if a patient has appropriate clinical findings within six hours of a transfusion • Exclude of other causes of pulmonary edema • Cardiac causes • Volume overload • Clinical diagnosis
TRALI: Treatment and Prognosis • Ventilatory support as required • Maintenance of hemodynamic status • Inotropes, vasopressors • 80% of patients show clinical improvement within 48-96 hours • In most patients, there are no long-term complications • Fatal in 5-10% of cases
Differential Diagnosis of TR with SOB: Background • Transfusion-related acute lung injury (TRALI) • Circulatory overload (TACO) • Transfusion associated dyspnea (TAD) • Anaphylaxis • Acute hemolytic transfusion reaction • Bacterial contamination • Other etiology unrelated to transfusion
TACO • Acute pulmonary edema secondary to congestive heart failure precipitated by transfusion of a volume of blood greater than what the recipient’s circulatory system can tolerate • Respiratory distress and/or cyanosis associated with pulmonary edema within 6 hours of transfusion • Associated with hypertension, tachycardia, positive fluid balance • Many patients also complain of a dry cough, headache, chest tightness Bux J, Transfus Med Hemother 2008
TACO: Epidemiology • Likely the most under-recognized and potentially serious transfusion complication • Studies have demonstrated incidence in orthopedic surgery patients (hip or knee arthroplasty) to be 1-8% Bux J, Transfus Med Hemother 2008 Popovsky MA, Transfusion and Apheresis Science, 2006
TACO: Risk Factors • Too much blood transfused too rapidly • Can be precipitated by even a single RBC unit • Age <3 or >60 years • Diminished cardiac reserve • Chronic anemia Bux J, Transfus Med Hemother 2008
TACO: Treatment and Prevention Prevention • Transfuse only when indicated • Recognize patients at risk • If at risk, transfuse slowly • Consider diuretics (before and/or after) • Watch fluid balance, monitor patient closely Treatment • Stop transfusion • Position patient in upright position • Supplementary oxygen • Diuretics • Cardiac and respiratory support as required
Differential Diagnosis of TR with SOB: Background • Transfusion-related acute lung injury (TRALI) • Circulatory overload (TACO) • Transfusion associated dyspnea (TAD) • Anaphylaxis • Acute hemolytic transfusion reaction • Bacterial contamination • Other etiology unrelated to transfusion
Transfusion associated dyspnea (TAD) • European Haemovigilience Network (EHN) introduced term to allow for classification of respiratory distress temporally associated with transfusion which could not be assigned to known pulmonary reactions www.ihn-org.net
Differential Diagnosis of TR with SOB • Transfusion-related acute lung injury (TRALI) • Circulatory overload (TACO) • Transfusion associated dyspnea (TAD) • Anaphylaxis • Acute hemolytic transfusion reaction • Bacterial contamination • Other etiology unrelated to transfusion • Can you narrow the diagnosis down?
Immediate Management: TR with SOB • Stop transfusion immediately • Notify hospital blood bank of transfusion reaction • Sample sent: screen for hemolysis, DAT • Maintain IV access (0.9% saline) • Monitor patient’s vital signs • Recheck identification of patient (wrist band) and label of blood product for discrepancy • CXR
Serious Reaction • What symptoms/signs would suggest a serious reaction? • Hypotension/shock • Shortness of breath • Hypoxemia • Hemoglobinuria • Nausea and vomiting • Bleeding from IV sites • Back pain • Chest pain • Temperature >39oC
Initial management of a serious reaction with SOB • Suspect TRALI, TACO • Do not restart transfusion • Notify blood bank and hematologist on call • Maintain IV access • CXR • Assess patient • JVP, pulmonary edema: suspect TACO • Diuresis, supportive therapy • Normal JVP, fever, CXR suspicious for ALI: suspect TRALI • Supportive therapy
Approach to Patient with a Transfusion Reaction • 65 year old man develops fever (temp 38oC) with rigors and chills while receiving unit of PRBC. • What is the differential diagnosis?
Approach to acute transfusion reactions commonly presenting with fever
Differential diagnosis: TR with Fever • Acute hemolytic transfusion reactions (AHTR) • Febrile non-hemolytic transfusion reactions (FNHTR) • Bacterial sepsis or contamination • Transfusion-related acute lung injury • Etiology unrelated to transfusion Fever is usually the predominant symptom
Differential diagnosis: TR with Fever • Acute hemolytic transfusion reactions (AHTR) • Febrile non-hemolytic transfusion reactions (FNHTR) • Bacterial sepsis or contamination • Transfusion-related acute lung injury • Etiology unrelated to transfusion
AHTR • Lysis or accelerated clearance of red cells in a transfusion recipient due to immunologic incompatibility between the blood donor and the recipient • Antigen-positive red cells are transfused to a recipient who has incompatible alloantibodies • Results in intravascular hemolysis Epidemiology • Generally within the top 3 causes of transfusion-related mortality • 10.8% of all fatalities reported to the US FDA in 2005-2008
AHTR—Etiology • Often due to the administration of ABO incompatible blood • Cross-match error • wrong identification of blood specimen • blood administered to wrong patient • May rarely be due to recipient allo-antibodies to other red cell antigens • Other causes of hemolysis include: • Overheating of RBC • Freezing of RBC • Outdated RBC • Transfusion under pressure with small bore needle • Transfusion with hypotonic solution • Causes unrelated to transfusion
AHTR-- Pathophysiology • Red cell alloantibody (IgM) in recipient binds to antigen on transfused red cell membrane • Development of immune complexes and activation of complement • Results in formation of membrane attack complex (C5b-9) on the red cell surface which leads to lysis of cells • Release of C3a and C5a • Hypotension • Production of IL-1 from macrophages • Fever • Activation of coagulation cascade • Disseminated intravascular coagulation (DIC)
AHTR--Clinical Presentation • Acute onset, often within first 15 minutes of starting transfusion • Transfusion of as little as 20-30 mL of red cells may result in an acute hemolytic transfusion reaction • Initial clinical presentation: • Fever and/or chills, anxiety, nausea or vomiting, pain (flank, back, abdomen, chest, head, infusion site), dyspnea, hypotension, brown urine, bleeding • Complications: • Renal failure, disseminated intravascular coagulation (DIC), death
AHTR—Treatment • STOP the transfusion immediately • Begin infusion with normal saline • Alert the blood bank, check for clerical error, send entire transfusion set-up to blood bank for testing • Supportive care • Monitor vital signs closely • Maintain blood pressure and urine output • Monitor for hyperkalemia • Administer FFP, cryoprecipitate and platelets as required for coagulopathy
AHTR—Investigation • Clerical check (labels, records in blood bank, review of blood typing results, antibody tests) • Repeat ABO type • Post-reaction blood specimen • Visual check for free hemoglobin • DAT • ABO type • Antibody screen • Evidence of hemolysis • free serum hemoglobin, haptoglobin, LDH, urine free hemoglobin
Transfusion Reactions with Fever: Background • Acute hemolytic transfusion reactions (AHTR) • Febrile non-hemolytic transfusion reactions (FNHTR) • Bacterial sepsis or contamination • Transfusion-related acute lung injury • Etiology unrelated to transfusion
FNHTR—Epidemiology • Common adverse event • 1 in 10 transfusions of pooled random donor platelets • 1 in 3000 units of RBC • Frequency varies with: • Type of blood product • Age of blood product • WBC content of blood product • Recipient characteristics • Use of pre-medications • Variability in recording of symptoms Callum J, Pinkerton P. Bloody Easy, 2nd edition, 2005
FNHTR—Etiology Reactions mediated by antibodies • Recipient alloantibody reactive to antigens expressed on WBCs in component • Antigen-antibody interaction causes the release of endotoxins • 1o mechanism causing FNHTR after transfusion of RBC Reactions mediated by biologic response molecules • Accumulation of leukocyte and/or platelet-derived cytokines in the bag during storage • IL-1b, IL-6, IL-8, TNF-a • Accounts for >90% of reactions to platelet transfusions Heddle et al., 1994; Brittingham and Chaplin, 1957; deRie et al., 1985; Perkins et al., 1966; Heddle et al., 1994; Muylle and Peeterman, 1994; Stack and Snyder, 1994; Aye et al.,1995; Kluter et al., 1995; Flegel et al., 1995.
FNHTR—Clinical Presentation • Fever (>1oC rise) during or soon after transfusion • Usually associated with chills and rigors • May be associated with nausea and vomiting • Symptoms typically appear toward the end of the transfusion • 5-10% of reactions present 1-2 hours after the transfusion AABB Technical Manual, 14th Edition, 2002; Heddle et al., 2002; Heddle et al., 1993.
FNHTR—Treatment • Stop the transfusion while assessing patient • Determine that an acute hemolytic transfusion reaction or reaction secondary to bacterial contamination is not occurring • Acetaminophen +/- merperidine may help patients with severe chills and rigors • Continue transfusion cautiously
Transfusion Reactions with Fever: Background • Acute hemolytic transfusion reactions (AHTR) • Febrile non-hemolytic transfusion reactions (FNHTR) • Bacterial sepsis or contamination • Transfusion-related acute lung injury • Etiology unrelated to transfusion