Download
1 / 1
10 likes | 100 Views
Comprehens ive Management of Hepatitis B Pregnancies in a Community Health Setting: The Hepatitis B Moms Program. Su Wang, MD, MPH 1 , Alice H. Tin, MPH 1 , Angelica Sze 1 , Calvin Yu 1 , Jennifer Lau 1 , Sherry Huang, MD 1 , Calvin Pan, MD 2

E N D
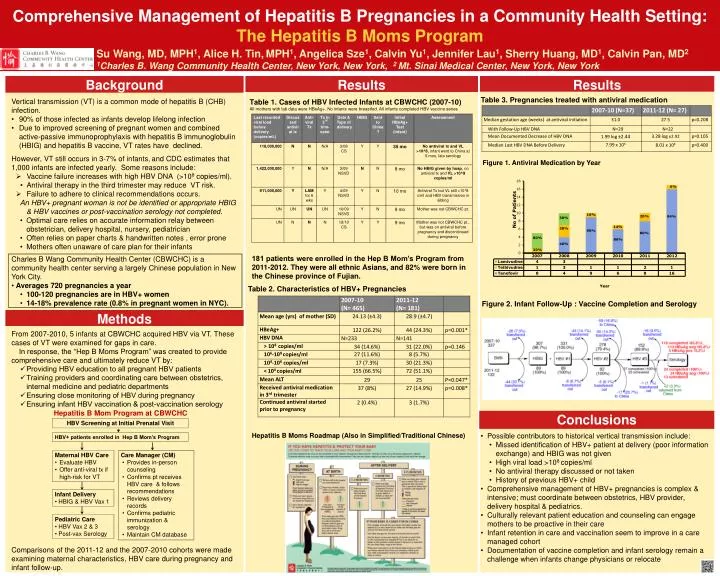
Comprehensive Management of Hepatitis B Pregnancies in a Community Health Setting: The Hepatitis B Moms Program Su Wang, MD, MPH1, Alice H. Tin,MPH1, Angelica Sze1, Calvin Yu1, Jennifer Lau1, Sherry Huang, MD1, Calvin Pan, MD2 1Charles B. Wang Community Health Center, New York, New York, 2 Mt. Sinai Medical Center, New York, New York AASLD Poster # Background Results Results Table 3. Pregnancies treated with antiviral medication • Vertical transmission (VT) is a common mode of hepatitis B (CHB) infection. • 90% of those infected as infants develop lifelong infection • Due to improved screening of pregnant women and combined active-passive immunoprophylaxis with hepatitis B immunoglobulin (HBIG) and hepatitis B vaccine, VT rates have declined. • However, VT still occurs in 3-7% of infants,and CDC estimates that 1,000 infants are infected yearly. Some reasons include: • Vaccine failure increases with high HBV DNA (>108 copies/ml). • Antiviral therapy in the third trimester may reduce VT risk. • Failure to adhere to clinical recommendations occurs. • An HBV+ pregnant woman is not be identified or appropriate HBIG & HBV vaccines or post-vaccination serology not completed. • Optimal care relies on accurate information relay between obstetrician, delivery hospital, nursery, pediatrician • Often relies on paper charts & handwritten notes , error prone • Mothers often unaware of care plan for their infants • Charles B Wang Community Health Center (CBWCHC) is a community health center serving a largely Chinese population in New York City. • Averages 720 pregnancies a year • 100-120 pregnancies are in HBV+ women • 14-18% prevalence rate (0.8% in pregnant women in NYC). • From 2007-2010, 5 infants at CBWCHC acquired HBV via VT. These cases of VT were examined for gaps in care. • In response, the “Hep B Moms Program” was created to provide comprehensive care and ultimately reduce VT by: • Providing HBV education to all pregnant HBV patients • Training providers and coordinating care between obstetrics, internal medicine and pediatric departments • Ensuring close monitoring of HBV during pregnancy • Ensuring infant HBV vaccination & post-vaccination serologyHepatitis B Mom Program at CBWCHC • Comparisons of the 2011-12 and the 2007-2010 cohorts were made examining maternal characteristics, HBV care during pregnancy and infant follow-up. Table 1. Cases of HBV Infected Infants at CBWCHC (2007-10) All mothers with lab data were HBeAg+. No infants were breastfed. All infants completed HBV vaccine series Figure 1. Antiviral Medication by Year 181 patients were enrolled in the Hep B Mom’s Program from 2011-2012. They were all ethnic Asians, and 82% were born in the Chinese province of Fujian. Table 2. Characteristics of HBV+ Pregnancies Figure 2. Infant Follow-Up : Vaccine Completion and Serology Methods Conclusions HBV Screening at Initial Prenatal Visit Hepatitis B Moms Roadmap (Also in Simplified/Traditional Chinese) • Possible contributors to historical vertical transmission include: • Missed identification of HBV+ patient at delivery (poor information exchange) and HBIG was not given • High viral load >108 copies/ml • No antiviral therapy discussed or not taken • History of previous HBV+ child • Comprehensive management of HBV+ pregnancies is complex & intensive; must coordinate between obstetrics, HBV provider, delivery hospital & pediatrics. • Culturally relevant patient education and counseling can engage mothers to be proactive in their care • Infant retention in care and vaccination seem to improve in a care managed cohort • Documentation of vaccine completion and infant serology remain a challenge when infants change physicians or relocate HBV+ patients enrolled in Hep B Mom’s Program • Maternal HBV Care • Evaluate HBV • Offer anti-viral tx if high-risk for VT • Care Manager (CM) • Provides in-person counseling • Confirms pt receives HBV care & follows recommendations • Reviews delivery records • Confirms pediatric immunization & serology • Maintain CM database • Infant Delivery • HBIG & HBV Vax 1 • Pediatric Care • HBV Vax 2 & 3 • Post-vax Serology






















