Download
1 / 21
220 likes | 304 Views
Two Models and the Outcomes. Ingrid Wagner, PhD. Background References.

E N D
Two Models and the Outcomes Ingrid Wagner, PhD.
Background References • Wagner, I., Munt, G. & Briner, P. (2006). Introducing Evidence-Based Family Assessment and Therapy in Child and Youth Mental Health Services: Applying Systemic Principles to Maintain, Sustain and Build Capacity. Australian and New Zealand Journal of Family Therapy, 27, 4, pp. 187-198. • Beavers, W. Robert & Hampson, Robert B. (1990). Successful Families. Assessment and Intervention. W.W. Norton and Company Inc. New York.
History of Family Typology/Paradigm Research • Etiologic Models – • Family types • “alcoholic family” • “schizophrenic family” • Structural Models – • enmeshed and disengaged family structure • Families of the Slums – dispelled the myth that poverty was synonymous with disorganization, and upheld the principle of equifinality
History of Family Typology/Paradigm Research • Transactional Models – David Reiss • No assumption of a causal link between family structure and illness behavior – neither the family nor the symptomatic individual can be identified as the location of the illness/disorder • consensus sensitive • Made up of enmeshed members who perceive the world as so chaotic and confusing that they must join together, maintain agreement at all times and protect themselves from danger • interpersonal distance sensitive • Made of disengaged individuals – “loners”- who strive to demonstrate their autonomy; attention to the suggestions or observations of others is a sign of weakness • environment sensitive • Made of members who believe the world is knowable and orderly and expect each member to contribute to its understanding and mastery
History of Family Typology/Paradigm Research • Process Models • Address the questions • Do families move from one category to another? • Is it possible for families to change typologies? • If so, is there an order to the way families change? • Are there levels of organization through which families, if they do change must pass or can families shift from one to any of the other categories?
Advantages of using a model in formal service settings • Supported by evidence – gives credibility to process • Gives direction to treatment planning and intervention • Assessment procedure standardized to be a consistent process across sites – good fit with current practice • Enables a shared understanding and common language of assessment • Enables the collection of both qualitative and quantitative data
Beavers Family Assessment System • Clinician Rating Instruments • Beavers Interactional Scales: Family Competence • Beavers Interactional Scales: Family Style • Family Self-Rating Instruments • Self-Report Family Inventory (SFI) Version II • Ages 11 years and over.
The Assumptions of the Beavers’Assessment • Family functioning, in terms of systemic qualities of relationships, communication, and exchanges, takes precedence over form or typology. • Attempting to identify or label clinical typologies of symptomatic families (such as "the schizophrenogenic family") yields little useful information. Instead, functional and behavioural qualities of the unique system must be assessed. • Family competence, ranging from healthy family functioning to severely dysfunctional, is viewed along a progressive continuum, rather than in categorical typologies. • This helps us to assume a potential for growth and adaptation in all families. • Families at similar competence levels may show different functional styles of relating and interacting. • Most competent families are able to balance and shift their functioning styles as developmental changes occur. • The successful therapist achieves an understanding of the presenting family and subtly alters such factors as therapeutic orientation, power differential, and operating style to join the family and catalyze its growth. • The successful therapist also appreciates the hierarchical structure of interacting systems within and surrounding the family, ranging from the biological/cellular through the individual to higher-order systems, including extended family and larger social networks. • While direction intervention with any one specific level or all levels may not be necessary in any given case, ignoring potentially important biochemical, neurological, or larger systems influences may lead to failure. • Individual treatment for relationship difficulties, including but not limited to marital or parent-child relationships, is often ineffective and complicating procedure.
The Assumptions of the Beavers’Assessment Our premise is that we must understand family system operation, competence, and style in order to test our explicit assumptions, choose a therapeutic stance, perhaps alter that stance as the family gains competence, and then extricate ourselves from the family (Beavers & Hampson 1990).
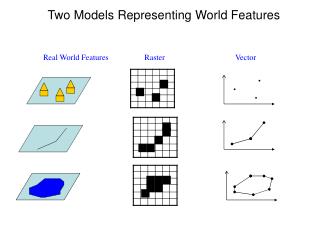
Diagram of Family Assessment Schema Competence Severely Dysfunctional Midrange Borderline Adequate Optimal 5 Centrifugal Often sociopathic offspring Often borderline offspring Often behaviour disorders 4 Style 3 Mixed 2 Often neurotic offspring Often severe obsessive/anorexic offspring Often schizophrenic offspring Centripetal 1 10 9 8 7 6 5 4 3 2 1
Relatively clear communication, constant effort at control, “loving means controlling”, distancing anger, anxiety or depression, ambivalence handled by repression Relatively clear boundaries, negotiating but with pain, ambivalence reluctantly recognized; some periods of warmth and sharing interspersed with control struggles Poor boundaries, confused communication, lack of shared attentional focus, stereotyped family process, despair, cynicism, denial of ambivalence Shifting from chaotic to tyrannical control efforts, boundaries fluctuate from poor to rigid, distancing, depression, outbursts of rage Capable negotiation, individual choice and ambivalence respected, warmth, intimacy, humour Severely Dysfunctional Borderline Midrange Adequate Optimal 5 Centrifugal Often sociopathic offspring Often borderline offspring Often behaviour disorders 4 3 Mixed 2 Often neurotic offspring Often severe obsessive/anorexic offspring Often schizophrenic offspring Centripetal 1 10 9 8 7 6 5 4 3 2 1
CP Borderline/SD functioning families • Restructuring, redefining roles, increasing coherent encounter, and helping individual family members resolve ambivalence are vital • Control is a theme- experience enough success to keep trying - • Families do not come to therapy because they are controlling. The come because they want to control things and are notably unsuccessful • The dilemma for the most overtly controlling member of the family is that what they want to control in the family relationship requires the other person’s choice
CP Borderline/SD functioning families • Important to keep in mind that everyone is hurting and not to become ensnared in “rescuing” the victim from the persecutor. • Attempting to rescue the “scapegoat” or victim in this process will not help to realign the family system, rather the therapist has been coopted by the system • To support change the therapist must maintain a meta-position
CP Borderline/SD functioning families • It is important to join with the family by not attempting to reshuffle its overt power structure. • Ambivalence in individuals is isomorphic with conflict in families – inevitable and ubiquitous. • Family rules can make it difficult for members to resolve mixed feelings – therefore therapists must make an effort to be the voice for denied opposites. • The therapist does not require a large overt power difference for effective work – initially the therapist needs to organize and structure a previously chaotic and incoherent situation • Empowerment of family members through the development of greater skills in negotiation is a key goal, and modelling by the therapist is a basic tool
CF Borderline/SD functioning families • Centrifugal family members do not trust words or therapists, they are open in their conflicts but deny warmth, fear and human needs • It is hard to get the whole family together, and it is also frequently hard to define the number of person in the family – clinically it is important to understand that helping the family clearly to define its members is not only useful but necessary; at times it is a procedure that effectively treats the family • Ambivalence is denied but therapists must tease out positive feelings rather than negative ones – family members discover love, not anger. • Positive reframing is an important tool – redefining behavioral chaos and aggressive, challenging provocations as grief, fear and neediness has at least 2 values – since it may be true it allows the other side of ambivalence to be voiced, the vulnerable is acknowledged and addressed. Second it attaches to unwanted behaviour a motivation that is frequently so distasteful to the perpetrator that the behaviour is derailed or inhibited.
CF Borderline/SD functioning families • Centrifugal family members do not enjoy each other very much. They look for satisfaction outside the family. One measure of recovery is the discovery that one can have good times at home. • To facilitate good times, memories of early enjoyments can be elicited from parents or children - it is easier to admit softness, hunger, and need if tender moments and feelings are couched in each family member’s childhood memories, rather than the present. • Limit-setting in sessions is most important, the therapist must keep order or insist that the parents keep order to develop behavioural coherence. Accepting behavioural chaos is not useful – therapists should consider splitting up the family members and undertaking separate work with the family subsystems • Therapy may include a lot of teaching to support appropriate power for parents and communication skills to reduce chaos
Current Models • Evidence-Based Model • Focus on diagnosis/disorder • Arise from clinical work and hypothesized models • Tested for effectiveness • Characteristics • Principle based – the therapist must adopt the stance • Draw on multiple theories • Describe Phases of Change
Family Based Approach for Anorexia Nervosa The five tenets of family-based treatment • An agnostic position in regard to the causes of AN – neither the child nor the parents are to blame • Empowerment – parents are central to the recovery of their child • Separate the child from the illness – externalize the Anorexia Nervosa • Non-authoritative therapeutic stance – the therapist joins with the family • The initial focus is on the symptoms of the Anorexia Nervosa
Attachment Based Family Therapy for Adolescent Depression/Suicidality The five tasks • Relational Reframe - Attributional shift in how family members view the problem and solution • Adolescent alliance – Better understanding of attachment narrative (i.e. Thoughts, feelings memories – revival of desire for and willingness to negotiate attachment) • Parent alliance – Shift in the parents’ working model of the adolescent and their parenting role (Acquisition of emotion coaching skills) • Repairing attachment – Engage in conversations that work through attachment ruptures (revise the view of self and other, and renew interpersonal trust) • Promoting autonomy – Parents effectively help adolescents resolve non-family based problems (depression, school, emerging self-identity – resumption of negotiation of adolescent development)
Jessie • 16 yr old male with 1 year history of Anorexia Nervosa • Referred following inpatient treatment for weight restoration • Treated with FBT – good progress until Phase 2 >90% EBW – suicide attempts x 3 • Transition to ABFT • Disclosed gender preference