Download
1 / 27
280 likes | 793 Views
Renal and Hepatic Impairment and Drug Dosing Med-III Core Clinical Pharmacology. Robert E. Ariano, Pharm.D., BCPS, FCCM Associate Professor of Pharmacy & Medicine, Critical Care Pharmacist, Department of Pharmacy, St. Boniface General Hospital & Department of Pharmacology & Therapeutics,

E N D
Renal and Hepatic Impairment and Drug DosingMed-III Core Clinical Pharmacology Robert E. Ariano, Pharm.D., BCPS, FCCM Associate Professor of Pharmacy & Medicine, Critical Care Pharmacist, Department of Pharmacy, St. Boniface General Hospital & Department of Pharmacology & Therapeutics, University of Manitoba
Renal Impairment Goals: Using pharmacokinetic (PK) principles to assist your decision on when to alter drug dosing based on the degree of renal impairment Estimate the creatinine clearance of your patient from their age, gender, and serum creatinine Establish a dosage regimen for a patient with known renal function impairment
Principles: The normalized creatinine clearance formulae is: CrCl = (140-Age) * 88.4 = 120 mL/min/1.73m2 (s-Creatinine umol/L) 85% of this value for females D’Angio R, Platt DR, Gannon R. Creatinine clearance: corrected vs uncorrected. Drug Intelligence & Clinical Pharmacy 1988;22:32-33
Case #1:Drug dosing in the renally impaired patient A 45 yo, 80 kg male patient with intra-abdominal sepsis is to receive gentamicin Normally he would receive 2 mg/kg load, then 1.5 mg/kg q8h with normal renal function, however, his serum creatinine is 220 umol/L ! a). What is the percentage of gentamicin excreted unchanged by the kidneys? 100% 100%
Estimate Patient’s GFR: b). What is this patient’s estimated creatinine clearance? CrCl = (140- 45 yo) * 88.4 ( 220 umol/L) = 38 mL/min/1.73m2 = 38 mL/min/1.73m2
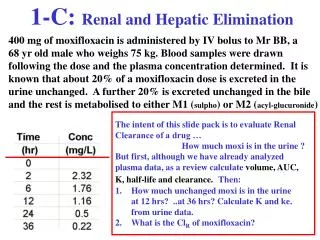
Use of the dosing nomograms: c). How would you adjust the antimicrobial dosing regimen for this patient’s level of renal dysfunction? Report the answer in milligrams per kilogram KEY POINT: His renal dysfunction will cause a retention and accumulation of the drug if you were to continue using a dosing regimen unadjusted for his poor drug elimination!
The concentrations achieved with normal renal function Desired Trough < 1.5 mg/L Gentamicin 160mg i.v. load, then 120mg i.v. q8h e.g. patient’s creatinine = 70 umol/L Creatinine clearance = 120 mL/min/1.73m2
Drug accumulation with renal dysfunction! Desired Trough < 1.5 mg/L Gentamicin 160mg i.v. load, then 120mg i.v. q8h e.g. patient’s creatinine = 220 umol/L Creatinine clearance = 38 mL/min/1.73m2
Traditional Gentamicin dosing: The Loading Dose 1.5 – 2 mg/kg total body weight [TBW]
Modified Sarubbi-Hull Nomogram for maintenance dose: %-age of loading dose required for dosage-interval selected 38 Sarubbi-Hull, Ann Intern Med 1976;85:183
Traditional Gentamicin dosing:The Maintenance Dose From the table therefore: MD = 90% of the load IV q24h ie. 2 mg/kg * 0.90 = 1.8 mg/kg IV q24h
Writing the orders: Thus a45 yo,80 kg male patient; and a CrCl of 38 mL/min/1.73m2 requires… Gentamicin 160 mg IV load,(2mg/kg)then 140 mg IV q24h(1.8mg/kg)
The results of your dosing adjustment on levels! Desired Trough < 1.5 mg/L Gentamicin 160mg i.v. load, then 140mg i.v. q24h e.g. patient’s creatinine = 220 umol/L Creatinine clearance = 38 mL/min/1.73m2
Additional considerations: • calculate as a percentage of the load (1.5-2 mg/kg of TBW or ‘Dosing Body Weight’ if obese) • round off dose to nearest 10 mg • if CrCl < 15 mL/min/1.73m2 or hemodialysis – give the same loading dose, but check morning levels after 48 hours to assist with dosing. Once less than 1.5 mg/L, then give 1 mg/kg as a single bolus, and again repeat levels in 48 hours
Case #2:Drug dosing in the renally impaired patient A 65 yo female patient with a hospital-acquired Pseudomonas aeruginosa pneumonia. She has renal dysfunction with a serum creatinine at 160 umol/L. a). What percentage of ceftazidime is excreted unchanged by the kidneys? 90%
Estimate Patient’s GFR: b). What is this patient’s estimated creatinine clearance? CrCl = (140- 65 yo) * 88.4 * 85% ( 160 umol/L) c). How would you adjust the antimicrobial dosing regimen for this patient’s level of renal dysfunction? = 35 mL/min/1.73m2
Writing the orders: Thus a 65 yo, 70 kg female patient; and a CrCl of 35 mL/min/1.73m2 requires… Ceftazidime 1.5 g IV q12h
Hepatic Impairment Principles: Influences of hepatic function on drug pharmacokinetics are not as clearly defined Wide inter-patient variability in hepatic drug elimination exists even in the presence of normal liver function A variety of pathophysiologic changes occur in liver disease: alterations in hepatic blood flow, biliary flow, hepatic shunting, enterohepatic cycling, and reductions in drug binding proteins
Hepatic Impairment - Take Home: Although alterations in drug PK’s are clearly dependent on the severity of the hepatic disease, they are frequently unpredictable Drug dosing in hepatic impairment is still very empiric, but may be assisted if an ability to measure serum drug concentrations is available
Hepatic Impairment • Research has shown reduced drug-metabolizing enzyme (CYP & conjugation reactions) in cirrhotics with worsen disease severity (Child-Pugh score), but with large variability! • But Conjugation < < Phase-I Oxidative reactions • Preferentially recommend conjugatively metabolized agents in cirrhotics • In the absence of recommended doses: • Child-Pugh A - Reduce maintenance to 50% • Child-Pugh B - Reduce maintenance to 25% • Child-Pugh C - Proven safe, or level monitoring available
Questions? Grand Beach July 2006
Aminoglycosides:When to obtain Peak and Trough Levels Obtain pre and post levels after the 3rd or 4th dose (whenever convenient for phlebotomy service). This reflects about 4 to 5 half-lives for these agents. Trough Goals: 0.5 – 1.5 mg/L (immediately pre- or within 45 minutes of the schedule dose) Peak Goals: 6 – 10 mg/L (20 – 30 minutes after end of infusion) Gent 100mg load, & 80mg q8h
Aminoglycoside toxicity assessment: Nephrotoxicity – Check aminoglycoside levels twice weekly. Monitor serum creatinines daily in unstable patients and 3 times weekly in stable patients - a change in creatinine of greater than 40 umol/L in 3 days is considered very significant Otovestibular Toxicity – If a patient requires an aminoglycoside for greater than 7 days, question the patient for the presence of dizziness, tinnitus, fullness in the head, pressure or pain in the ears, double-vision, or diminished hearing
‘High-Dose’ Single daily dose of 6 mg/kg IV eg. 420 mg IV gentamicin Normal Renal Function CrCl = 100 mL/min/1.73m2 Trough range associated with nephrotoxicity
High-dose or ‘Once-Daily’ aminoglycosidesRecommendations… • give a single 420 mg gentamicin dose IV over 1 hour • request a trough gentamicin level in 24 hours • if trough less than 1 mg/L, the drug can be continued Is NOT for everyone; avoid in… • burns, cystic fibrosis, pregnancy, pediatrics, endocarditis, & in renal insufficiency (ie. serum creat. > 110 umol/L)