Download
1 / 33
350 likes | 758 Views
Direct Ophthalmoscopy. “THE EYE IS A WINDOW TO SYSTEMIC DISEASE”. Sandra Tubito, O.D. July 2007. Discussion Outline. Why ophthalmoscopy? Types of ophthomoscopy Direct ophthalmoscope Examination Procedure Setting External Exam Internal Exam What you should see Pathology Questions.

E N D
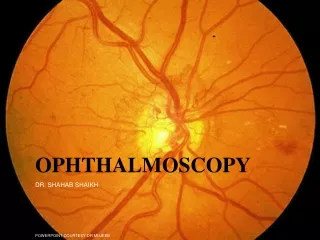
DirectOphthalmoscopy “THE EYE IS A WINDOW TO SYSTEMIC DISEASE” Sandra Tubito, O.D. July 2007
Discussion Outline • Why ophthalmoscopy? • Types of ophthomoscopy • Direct ophthalmoscope • Examination Procedure • Setting • External Exam • Internal Exam • What you should see • Pathology • Questions
Why ophthalmoscopy? • Only way (and place in the body) that veins and arteries can be seen in their natural state, non-invasively. • Part of general optical screening where direct observation of the structures of the fundus may show: • Disease of the eye itself (e.g. glaucoma, retinal detachment) • Abnormalities indicative of disease elsewhere in the body (e.g. diabetes, hypertension) • Evaluation of ocular complaints
Types of Ophthalmoscopes Direct ophthalmoscope Indirect ophthalmoscope
Direct X15 magnification 10° field of view Real image Monocular Undilated pupil Maximum resolution of 70µm Indirect X2-3 magnification 30° field of view Inverted and upside down image Binocular Dilated pupil Maximum resolution of 200µm Types of Ophthalmoscopes
Direct Ophthalmoscope • Illuminating system • Light bulb • Lenses • Reflector • Aperture stops and filters • Different sized stops to change illumination of the retina • Green (red free) filter • Viewing system • Sight hole (3mm in diameter) • Focusing lenses
Examination Procedure • Setting • Dark room • Seat patient in comfortable chair with head rest • Ask patient to look at a slightly elevated target on opposite wall
Examination Procedure • External Exam • Look at R eye with R eye (L with L) • Place hand on shoulder or forehead • Change viewing angle to 15° to avoid light reflex of cornea
Examination Procedure • External Exam • Red Reflex - hold ophthalmoscope at ~50cm and look through sight hole at the ocular media. Find the red reflex in the pupil. Opacities (eg cataracts) can be seen. • Place +8.00D lens in sight hole and move to ~10cm to inspect anterior structures: • lids/lashes • conjunctiva • cornea
Examination Procedure • Internal Exam • Turn focus wheel to bring anterior chamber and iris into focus • Gradually reduce power in ophthalmoscope to focus on internal structures: • Lens • Vitreous • Retina
Examination Procedure • Internal Exam • Continue turning focus wheel to bring retina/vessels in focus • Follow the vessels to the disc • The ‘arrow’ point to the disc • Examine the disc, vessels, retina, & macula.
Things you should see • The optic nerve head • Appearance – shape/size (1.5mm in diameter) • Color – disc is pale pink, cup is whitish • Elevation – should be flat • Rim – clear and distinct • Cup/Disc ratio • Ratio of the diameter of the cup to the diameter of the disc
Things you should see • Retinal vessels • Arteries • Lighter in color, smaller • Veins • Darker in color, larger • May spontaneously pulsate at the disc (80%) • The ratio of the artery :vein diameter is normally ~ 2:3 • Follow vessels from disc • Look at arterio-venous crossings for abnormalities (nicking, compression, elevation, deviation) • Check arterial light reflex. This will get whiter and thicker in arteriosclerosis
Arteriovenous changes Tapering concealment of the vein appearing as ‘nicking’ Elevation of the vein over the artery Deviation of the vein out of its path Compression of the vein at the arterio-venous crossing, causing stenosis of the distal vein
Things you should see • Retina • Check the background retina • Look for color differences • areas of hyper or hypo pigmentation • Scarring • Raised areas • Hemorrhages, microaneurisms • Cotton wool exudates • Hard exudates • A more peripheral view can be obtained by having the patient look in different directions OD OS
Things you should see • Fovea and Macula • Change sight hole to the smallest aperature • Have patient look at the light • Temporal and slightly inferior to the disc • Slightly darker than rest of retina • Central depression/reflex - fovea
Pathology - The optic nerve Optic atrophy
Pathology - The optic nerve “Choked disc” or Papilledema
Pathology – The optic nerve Glaucomatous cupping
Pathology - The optic nerve Papilledema with papillary hemorrhages Disc neovascularization
Pathology – Retina / Vessels Arterial occlusions
Pathology – Retina / Vessels Circinate exudates
Pathology – Retina / Vessels Intra-retinal hemorrhages
Pathology – Retina / Vessels Cotton wool spots
Pathology – Retina / Vessels Neovascularization
Pathology - Retina / Vessels Arterial plaques
Pathology – Retina / Vessels Venous occlusions
Pathology - Macula Drusen
Pathology - Macula Age related macula degeneration Hemorrhagic phase
Pathology - Macula Exudative age related macular degeration