Download
1 / 37
400 likes | 629 Views
Colhoun. HM et al. Lancet. 2004;364:685. -. 696. INTERHEART: Risk of Acute Myocardial Infarction associated with self-reported diabetes. Overall and Region-by-Region Odds ratio after adjusting for age, sex and smoking. Myocardial perfusion in diabetic patients.

E N D
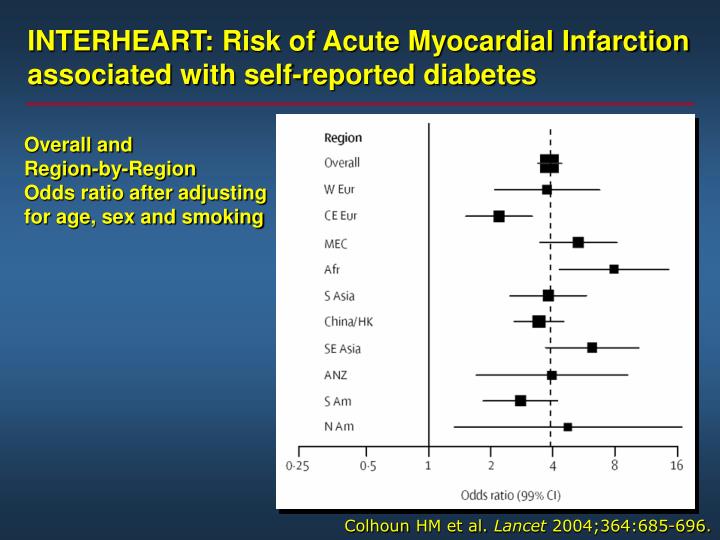
Colhoun HM et al. Lancet 2004;364:685 - 696. INTERHEART: Risk of Acute Myocardial Infarction associated with self-reported diabetes Overall and Region-by-Region Odds ratio after adjusting for age, sex and smoking
Protein Kinase Cb Isoform InhibitorsA New Treatment for Diabetic Cardiovascular Diseases Insulin resistance Hyperglycemia Atherosclerosis, Diabetes, Microvascular Complications, Cardiomyopathy He et al. Circulation 2004;110:7-9
by Alexander 2003 Age-adjusted prevalence of metabolic syndrome in the U.S. population over 50 years of age categorized by glucose intolerance (NFG, normal fasting glucose; IGT, impaired glucose tolerance without impaired fasting glucose; IFG, impaired fasting glucose with or without impaired glucose tolerance; DM, diabetes mellitus).
Approaches to the Treatment of the Metabolic Syndrome
Trials of Dietary Interventions and Coronary Events(adapted from Hu 2002)
INTERHEART: Decreased Risk of AMI with Avoidance of Smoking; Daily Fruits/ Veg , Reg Phys Activity & Alcohol 0.35 0.70 0.86 0.91 0.24 0.21 0.19 1.0 0.5 OR (99% CI) 0.25 0.125 no Frt / Veg Nosmk Exer Alc + exer + alc smk Smk = smoking DM = diabetes HTN = hypertension Obes = obesity Ps = psychosocial factors Note: odds ratio plotted on a doubling scale + fvg Yusuf S et al. Lancet. 2004;364:937-52.
Magnitude of cardiovascular risk reductions (relating to primary cardiovascular endpoints) in selected major intervention trials evaluating lipid-lowering, antihypertensive or oral antidiabetic therapies. Adapted from data presented by Libby and Plutzky (2002)
UKPDS Confirmed: Metformin Reduces Risk of Macrovascular Complications (independent of improvement in glycaemic control) Any diabetes-related Diabetes- related death All cause mortality Myocardial infarction Macrovascular 0 5 10 15 20 % risk reduction 25 30 P=0.020 35 P=0.0023 P=0.011 40 P=0.010 45 P=0.017 50 Metformin in overweight (>120% ideal body weight) patients UKPDS 34. Lancet 1998; 352: 854-865
INTERHEART: Impact of multiple risk factorson CV risk 2.9 2.4 1.9 3.3 13.0 42.3 68.5 182.9 333.7 512 256 128 Odds ratio for1st MI (99% CI) 64 32 16 8 4 2 1 Smk(1) DM(2) HTN(3) ApoB-ApoA1(4) 1+2+3 All 4 All 4+ Obes All 4+ Ps All riskfactors Smk = smoking DM = diabetes HTN = hypertension Obes = obesity Ps = psychosocial factors Note: odds ratio plotted on a doubling scale Yusuf S et al. Lancet. 2004;364:937-52.
Lipids and Lipoproteins in Patients With Type 2 Diabetes Smaller VLDL LPL IDL LPL Large LDL TG pool Low LDL-R High Larger VLDL LPL LPL / HL Remnants Small LDL Smaller LDL HL Chol TG CETP HDL Smaller HDL Krauss et al. Diabetes Care 27:1496-1504, 2004
Stepwise selection of Risk Factors, adjusted for Age and Sex, in 2693 patients with Type 2 diabetes with Dependent Variable as Time to First Event UKPDS Group. Lancet 1998;352:837
CARDS: Effect of Atorvastatin on the Primary Endpoint: Major CV Events Including Stroke Relative Risk Reduction 37% (95% CI, 17–52)P = 0.001 15 Placebo127 events 10 Cumulative Hazard, (%) 5 Atorvastatin83 events 0 0 1 2 3 4 4.75 Years PlaceboAtorvastatin 14101428 13511392 13061361 10221074 651694 305328 Colhoun HM et al. Lancet 2004;364:685-696
CARD Study Effect of Treatment on Primary and Secondary endpoints. Colhoun HM et al. Lancet 2004;364:685-696
UKPDS - Blood Pressure Control Study any diabetes-related endpoint 24% diabetes-related deaths 32% stroke 44% microvascular disease 37% heart failure 56% retinopathy progression 34% deterioration of vision 47% in 1148 Type 2 diabetic patients a tight blood pressure control policy which achieved blood pressure of 144 / 82 mmHg gave reduced risk for:
MICRO-HOPE Primary Endpoints 25 RR=25% P<0.001 Placebo Ramipril 20 RR=22% P=0.01 15 RR=37% P<0.001 Events per patient group (%) RR=33% P=0.007 10 5 0 Combined primary endpoint* Myocardial infarction Stroke Cardiovascular death Lancet, 2000
HOT Trial:Cardiovascular Events in Diabetics and Nondiabetics—Effect of Diastolic Target at 4 Years 48% RiskReduction 24.4 18.6 Events / 1000 Pt-Years 11.9 9.9 10.0 9.3 <90 <85 <80 <90 <85 <80 DiabeticPatientsn=1,501; p=0.016 NondiabeticPatientsn=18,790; p=NS Hansson L et al. Lancet 1998;351: 1755-1762.
Risk of Diabetes Mellitus using ACEI, AT1 blockers, CCB, Diuretics and –blockers amorg Non Diaetic Subjects with Hypertension
Ridker 2003 Comparison of cardiovascular event-free survival for those with and without metabolic syndrome to those with baseline CRP levels above or below 3.0 mg/L. CVD indicates cardiovascular disease.
Antiplatelet Agents Reduce CVD Events in Patients with Diabetes: Antiplatelet Trialists’ Collaboration P<0.002 Antiplatelet Therapy Control P<0.00001 CVD Events (%) Diabetes No Diabetes Antiplatelet Trialists’ Collaboration. BMJ 1994;308:81-106.
Glycemic control A1C Preprandial capillary plasma glucose Peak postprandial capillary plasma glucose Lipids LDL Triglycerides HDL Blood Pressure < 7.0% 90-130 mg/dl (5.0-7.2 mmol/l) < 180 mg/dl (<10.0 mmol/l) < 130/80 mmHg < 100 mg/dl (< 2.6 mmol/l) < 150 mg/dl (< 1.7 mmol/l) > 40 mg/dl ( > 1.1 mmol/l) < 130/80 mmHg 2005 ADARecommendations for adults with diabetes
12 24 36 48 60 72 84 96 0 Composite Endpoint of Death from CV Causes, Nonfatal MI, CABG, PCI, Nonfatal Stroke, Amputation, or Surgery for PAD: STENO-2 60 Conventional Therapy p =0.007 50 Hazard ratio = 0.47 (95% CI, 0.24–0.73; P=0.008) 40 Primary Composite Endpoint (%) 30 20 Intensive Therapy 10 0 Months of Follow-up Gæde P et al. N Engl J Med 2003;348:383-393.
CV Outcomes in the Steno-2 Study STROKE MYOCARDIAL INFARCTION PCI or CABG Steno-2 Study – Diabetes 2004
CV Risk Reduction in the Steno-2 Study Steno-2 Study – Diabetes 2004
Efficacy of Multiple Risk Factor Intervention in High-Risk Subjects (Type 2 Diabetes with Microalbuminuria): Steno-2 Intensive Therapy Conventional Therapy 80 P=0.21 P<0.001 70 P=0.19 60 P=0.001 50 Patients Reaching Intensive-Treatment Goals at Mean 7.8 y, (%) 40 30 P=0.06 20 10 0 Glycosylatedhemoglobin <6.5% Cholesterol<175 mg/dl Triglycerides<150 mg/dl Systolic BP<130 mm Hg Diastolic BP<80 mm Hg Gæde P et al. N Engl J Med 2003;348:383-393.
Benefit from CV intervention and diabetes prevention • CV interventions (average percent benefit) • Glycemia 12% conventional(UKPDS) • Metformin 40% (wide CI - UKPDS) • Blood Pressure 20-40% (many studies) • ARB/ACE 25-30% (LIFE / HOPE) • Statin 22% - 42% (many studies) • Fibric acid 24% (DAIS / VA-HIT) • Aspirin 18-28% (ETDRS/Antiplat Collab) • Diabetes prevention • Lifestyle 58% (FPS / DPP) • Metformin 31% (DPP) • Acarbose 36% (STOP – NIDDM) • Troglitazone 55% (single center - TRIPOD) • Xenical 37% (XENDOS)