Download
1 / 10
100 likes | 258 Views
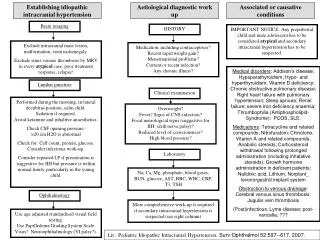
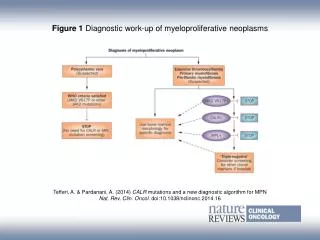
Diagnostic Work-up. Electroencephalography (EEG). The only diagnostic test for absence seizures Ambulatory EEG monitoring over 24 hours may be useful to quantitate the number of seizures per day and their most likely times of occurrence. EEG: Typical Absence.

E N D
Electroencephalography (EEG) • The only diagnostic test for absence seizures • Ambulatory EEG monitoring over 24 hours may be useful to quantitate the number of seizures per day and their most likely times of occurrence
EEG: Typical Absence • Findings in typical absence seizures include the following: • Background activity is normal. • In syndromes with frequent absence seizures, such as childhood absence epilepsy, a routine awake recording is often pathognomonic. • In syndromes with less frequent absence seizures (juvenile absence epilepsy or juvenile myoclonic epilepsy), an awake recording may be normal; a sleep or sleep-deprived recording may be needed. • Typical absence seizures have generalized 3-Hz spike-and-wave complexes
EEG: Typical Absence • The onset and ending of these seizures are abrupt; no postictal EEG slowing is noted. • Hyperventilation often provokes these seizures and should be a routine part of all EEGs in children. • EEG video monitoring demonstrates that clinical seizure manifestations may lag behind the start of ictal EEG activity; bursts lasting less than 3 seconds are usually clinically silent. • During the absence seizure, rhythmic eye blinks and mild clonic jerks may be present. As a seizure progresses, automatisms may be seen. • Clinical and EEG features may vary considerably in different children.
EEG: Atypical Absence • Findings in atypical absence seizures include the following: • Background activity is often abnormal, reflecting the diffuse or multifocal underlying encephalopathy of symptomatic generalized epilepsy. • Seizures are characterized by slow spike-and-wave paroxysms, classically 2.5 Hz.
EEG: Atypical Absence • The onset may be difficult to discern, and postictal EEG slowing may be noted. • The clinical correlation of generalized spike-and-wave complexes with clinical seizures is not as clear-cut as in typical absence seizures. • EEG-video monitoring can show a more varied alteration of consciousness than in typical absence seizures. If the patient has underlying mental retardation, discerning changes in mental status also may be more difficult in atypical absence. • Changes in postural tone, most noticeably head nods, are common.
Laboratory Studies • Laboratory tests for: • Metabolic abnormalities • Toxic or drug ingestion • Blood levels of electrolytes, glucose, calcium, magnesium • Hepatic or renal disease • If a clear history of the episodic nature of the attacks is obtained, then the EEG can be diagnostic and laboratory tests may not be necessary.
Imaging Studies • Neuroimagingis not indicated if the typical clinical pattern is present. • Neuroimaging findings are normal in idiopathic epilepsies by definition • Often ordered if a child presents with a generalized tonic-clonic seizure, to rule out significant structural causes of seizures. • If imaging is performed, MRI is preferred to CT scanning. MRI is more sensitive for certain anatomic abnormalities.