Download
1 / 14
140 likes | 262 Views
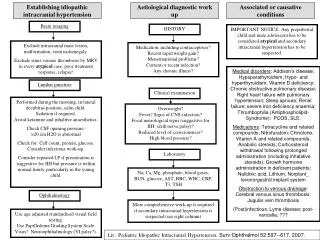
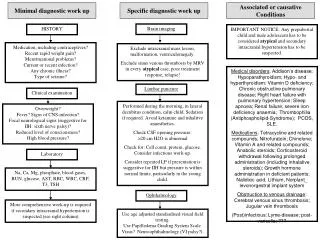
Diagnostic Work-Up. Imaging: X-Ray MRI UTZ. Cervical Spine Radiograph. Alignment is satisfactory Vertebral height is preserved Minimal osteophytes are seen in the cervical vertebral bodies There is a slight narrowing of the disk space at C5-C6, C6-C7

E N D
Diagnostic Work-Up • Imaging: • X-Ray • MRI • UTZ
Cervical Spine Radiograph • Alignment is satisfactory • Vertebral height is preserved • Minimal osteophytes are seen in the cervical vertebral bodies • There is a slight narrowing of the disk space at C5-C6, C6-C7 • The rest of the study is unremarkable
Cervical Spine Radiograph Impression: • Alignment is satisfactory • Vertebral height is preserved
Cervical Spine Radiograph Impression: • Minimal osteophytes are seen in the cervical vertebral bodies • There is a slight narrowing of the disk space at C5-C6, C6-C7 • The rest of the study is unremarkable
Cervical Spine Radiograph Impression: • Minimal osteophytes are seen in the cervical vertebral bodies • There is a slight narrowing of the disk space at C5-C6, C6-C7 • The rest of the study is unremarkable
Cervical Spine Radiograph Impression: • Minimal osteophytes are seen in the cervical vertebral bodies • There is a slight narrowing of the disk space at C5-C6, C6-C7 • The rest of the study is unremarkable
Cervical Spine Radiograph Impression: • Minimal osteophytes are seen in the cervical vertebral bodies • There is a slight narrowing of the disk space at C5-C6, C6-C7 • The rest of the study is unremarkable
Cervical Strain • caused most often by indirect trauma when the head is flung backward (hyperextension) or forward (hyperflexion) • Injuries caused by rotation and compression (when the force of impact lands on the top of the head) can also result in neck strains • Result of an abnormal posture while awake or asleep, repetitive or prolonged neck extension Childs, Cleland et al. 2008. Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2008;38(9):A1-A34. doi:10.2519/jospt.2008.0303
Addressing Neck Pain • Cochrane Collaboration Review of mobilization and manipulation for mechanical neck disorders included 33 randomized controlled trials of which 42% were considered high quality. • They concluded that the most beneficial manipulative interventions for patients with mechanical neck pain with or without headaches should be combined with exercise to reduce pain and improve patient satisfaction. Childs, Cleland et al. 2008. Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2008;38(9):A1-A34. doi:10.2519/jospt.2008.0303
Addressing Neck Pain • Manipulation (thrust) and mobilization (non-thrust manipulation) intervention alone were determined to be less effective than when combined with exercise (combined intervention) • A recently published clinical practice guideline concluded that the evidence for combined intervention was relatively strong, while the evidence for the effectiveness of thrust or non-thrust manipulation in isolation was weaker. Childs, Cleland et al. 2008. Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2008;38(9):A1-A34. doi:10.2519/jospt.2008.0303
Treatment of Neck Pain • July 2009: assessment if manual therapy (manipulation/mobilization), combined w/ exercise improves pain, function/disability, quality of life, global perceived effect, and patient satisfaction for adults with neck pain with or without cervicogenic headache or radiculopathy. • 2or more authors independently selected studies, abstracted data and assessed methodological quality. • Of 17 randomized controlled trials included, 29% had a low risk of bias. Miller J, Gross A et al. 2009. Manual therapy and exercise for neck pain: A systematic review.School of Rehabilitation Science, McMaster University, Hamilton, Canada. Man Ther. 2010 Jun 1.
Treatment of Neck Pain • High quality evidence suggests greater short-term pain relief than exercise alone, but no long-term differences across multiple outcomes for acute/chronic neck pain with or without cervicogenic headache. • Moderate quality evidence supports this treatment combination for pain reduction and improved quality of life over manual therapy alone for chronic neck pain • Low quality evidence suggests long-term improvement in pain, function/disability, and global perceived effect when manual therapy and exercise are compared to no treatment. • Evidence regarding radiculopathy was sparse Miller J, Gross A et al. 2009. Manual therapy and exercise for neck pain: A systematic review.School of Rehabilitation Science, McMaster University, Hamilton, Canada. Man Ther. 2010 Jun 1.
Impact of Osteoarthritis • June 2007: assessed the gender-related impact of OA on quality of life (QoL) and health service utilization of primary care patients in Germany. • Cross sectional study: 1250 OA patients attending 75 primary care practices from Mar-May 2005. • QoLwas assessed using the GERMAN-AIMS2-SF. • Data about comorbidities, prescriptions, health service utilization, and physical activity were obtained by questioning patients or from the patients' medical files. • Depression was assessed by means PHQ-9 Rossmann, Laux et al. 2007. Department of General Practice and Health Services Research, University of Heidelberg, Voßstrasse 2, 69115 Heidelberg, Germany. Osteoarthritis: quality of life, comorbidities, medication and health service utilization assessed in a large sample of primary care patients. Journal of Orthopaedic Surgery and Research 2007, 2:12doi:10.1186/1749-799X-2-12
Impact of Osteoarthritis • Impact of OA on QoL was different between gender: women achieved significantly higher scores in the AIMS2-SF dimensions lower body, symptom, affect and work. • 18.8 % of men and 19.7% of women had a concomitant depression • Women visited their physicians (mean 5.61 contacts in 6 months) more often than men (mean 4.08; p< 0.01) Rossmann, Laux et al. 2007. Department of General Practice and Health Services Research, University of Heidelberg, Voßstrasse 2, 69115 Heidelberg, Germany. Osteoarthritis: quality of life, comorbidities, medication and health service utilization assessed in a large sample of primary care patients. Journal of Orthopaedic Surgery and Research 2007, 2:12doi:10.1186/1749-799X-2-12