Download
1 / 1
10 likes | 97 Views
Research Database (ECRIC). Researchers Partners NHS. DELIVERY OF HIGH QUALITY MOLECULAR TESTS FOR 9,000 CANCER PATIENTS ROUTINELY CONSENTED FOR USE OF MOLECULAR AND CLINICAL DATA

E N D
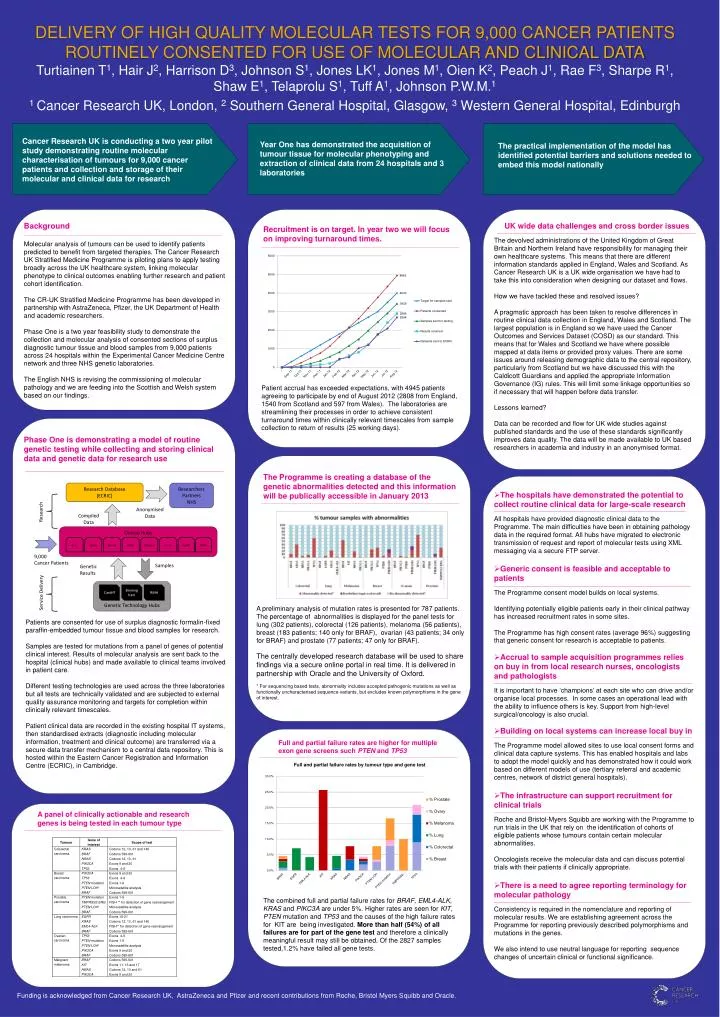
Research Database (ECRIC) Researchers Partners NHS DELIVERY OF HIGH QUALITY MOLECULAR TESTS FOR 9,000 CANCER PATIENTS ROUTINELY CONSENTED FOR USE OF MOLECULAR AND CLINICAL DATA Turtiainen T1, Hair J2, Harrison D3, Johnson S1, Jones LK1, Jones M1, Oien K2, Peach J1, Rae F3, Sharpe R1, Shaw E1, Telaprolu S1, Tuff A1, Johnson P.W.M.1 1 Cancer Research UK, London, 2 Southern General Hospital, Glasgow, 3 Western General Hospital, Edinburgh Anonymised Data Research Compiled Data Clinical Hubs 9,000 Cancer Patients Samples Genetic Results Year One has demonstrated the acquisition of tumour tissue for molecular phenotyping and extraction of clinical data from 24 hospitals and 3 laboratories Genetic Technology Hubs Cardiff Birmingham RMH Service Delivery The practical implementation of the model has identified potential barriers and solutions needed to embed this model nationally Background Molecular analysis of tumours can be used to identify patients predicted to benefit from targeted therapies. The Cancer Research UK Stratified Medicine Programme is piloting plans to apply testing broadly across the UK healthcare system, linking molecular phenotype to clinical outcomes enabling further research and patient cohort identification. The CR-UK Stratified Medicine Programme has been developed in partnership with AstraZeneca, Pfizer, the UK Department of Health and academic researchers. Phase One is a two year feasibility study to demonstrate the collection and molecular analysis of consented sections of surplus diagnostic tumour tissue and blood samples from 9,000 patients across 24 hospitals within the Experimental Cancer Medicine Centre network and three NHS genetic laboratories. The English NHS is revising the commissioning of molecular pathology and we are feeding into the Scottish and Welsh system based on our findings. UK wide data challenges and cross border issues Recruitment is on target. In year two we will focus on improving turnaround times. The devolved administrations of the United Kingdom of Great Britain and Northern Ireland have responsibility for managing their own healthcare systems. This means that there are different information standards applied in England, Wales and Scotland. As Cancer Research UK is a UK wide organisation we have had to take this into consideration when designing our dataset and flows. How we have tackled these and resolved issues? A pragmatic approach has been taken to resolve differences in routine clinical data collection in England, Wales and Scotland. The largest population is in England so we have used the Cancer Outcomes and Services Dataset (COSD) as our standard. This means that for Wales and Scotland we have where possible mapped at data items or provided proxy values. There are some issues around releasing demographic data to the central repository, particularly from Scotland but we have discussed this with the Caldicott Guardians and applied the appropriate Information Governance (IG) rules. This will limit some linkage opportunities so if necessary that will happen before data transfer. Lessons learned? Data can be recorded and flow for UK wide studies against published standards and the use of these standards significantly improves data quality. The data will be made available to UK based researchers in academia and industry in an anonymised format. Cancer Research UK is conducting a two year pilot study demonstrating routine molecular characterisation of tumours for 9,000 cancer patients and collection and storage of their molecular and clinical data for research Patient accrual has exceeded expectations, with 4945 patients agreeing to participate by end of August 2012 (2808 from England, 1540 from Scotland and 597 from Wales). The laboratories are streamlining their processes in order to achieve consistent turnaround times within clinically relevant timescales from sample collection to return of results (25 working days). Phase One is demonstrating a model of routine genetic testing while collecting and storing clinical data and genetic data for research use The Programme is creating a database of the genetic abnormalities detected and this information will be publically accessible in January 2013 • The hospitals have demonstrated the potential to collect routine clinical data for large-scale research • All hospitals have provided diagnostic clinical data to the Programme. The main difficulties have been in obtaining pathology data in the required format. All hubs have migrated to electronic transmission of request and report of molecular tests using XML messaging via a secure FTP server. • Generic consent is feasible and acceptable to patients • The Programme consent model builds on local systems. • Identifying potentially eligible patients early in their clinical pathway has increased recruitment rates in some sites. • The Programme has high consent rates (average 96%) suggesting that generic consent for research is acceptable to patients. • Accrual to sample acquisition programmes relies on buy in from local research nurses, oncologists and pathologists • It is important to have ‘champions’ at each site who can drive and/or organise local processes. In some cases an operational lead with the ability to influence others is key. Support from high-level surgical/oncology is also crucial. • Building on local systems can increase local buy in • The Programme model allowed sites to use local consent forms and clinical data capture systems. This has enabled hospitals and labs to adopt the model quickly and has demonstrated how it could work based on different models of use (tertiary referral and academic centres, network of district general hospitals). • The infrastructure can support recruitment for clinical trials • Roche and Bristol-Myers Squibb are working with the Programme to run trials in the UK that rely on the identification of cohorts of eligible patients whose tumours contain certain molecular abnormalities. • Oncologists receive the molecular data and can discuss potential trials with their patients if clinically appropriate. • There is a need to agree reporting terminology for molecular pathology • Consistency is required in the nomenclature and reporting of molecular results. We are establishing agreement across the Programme for reporting previously described polymorphisms and mutations in the genes. • We also intend to use neutral language for reporting sequence changes of uncertain clinical or functional significance. Birm Leeds Manch Edinb Glasgow Camb Cardiff RMH A preliminary analysis of mutation rates is presented for 787 patients. The percentage of abnormalities is displayed for the panel tests for lung (302 patients), colorectal (126 patients), melanoma (56 patients), breast (183 patients; 140 only for BRAF), ovarian (43 patients; 34 only for BRAF) and prostate (77 patients; 47 only for BRAF). The centrally developed research database will be used to share findings via a secure online portal in real time. It is delivered in partnership with Oracle and the University of Oxford. * For sequencing based tests, abnormality includes accepted pathogenic mutations as well as functionally uncharacterised sequence variants, but excludes known polymorphisms in the gene of interest. Patients are consented for use of surplus diagnostic formalin-fixed paraffin-embedded tumour tissue and blood samples for research. Samples are tested for mutations from a panel of genes of potential clinical interest. Results of molecular analysis are sent back to the hospital (clinical hubs) and made available to clinical teams involved in patient care. Different testing technologies are used across the three laboratories but all tests are technically validated and are subjected to external quality assurance monitoring and targets for completion within clinically relevant timescales. Patient clinical data are recorded in the existing hospital IT systems, then standardised extracts (diagnostic including molecular information, treatment and clinical outcome) are transferred via a secure data transfer mechanism to a central data repository. This is hosted within the Eastern Cancer Registration and Information Centre (ECRIC), in Cambridge. Failure rates are higher for the larger genes such as KIT, PTEN and P53 Full and partial failure rates are higher for multiple exon gene screens such PTEN and TP53 A panel of clinically actionable and research genes is being tested in each tumour type The combined full and partial failure rates for BRAF, EML4-ALK, KRAS and PIKC3A are under 5%. Higher rates are seen for KIT, PTEN mutation and TP53 and the causes of the high failure rates for KIT are being investigated. More than half (54%) of all failures are for part of the gene test and therefore a clinically meaningful result may still be obtained. Of the 2827 samples tested,1.2% have failed all gene tests. Funding is acknowledged from Cancer Research UK, AstraZeneca and Pfizer and recent contributions from Roche, Bristol Myers Squibb and Oracle.






















