Download
1 / 47
530 likes | 703 Views
Acute appendicitis. SURGICAL ANATOMY. Part of large intestine Size 7-10 cm long and lumen .2cm in diameter LOCATION Base is attached to posteriomedial aspect of cecum2.5 cm below the ileocecal junction Body n tip; Rectocecal 74% Pelvic 21% Paracecal 2% Subcecal 1.5% Preileal 1%

E N D
SURGICAL ANATOMY • Part of large intestine • Size 7-10 cm long and lumen .2cm in diameter • LOCATION • Base is attached to posteriomedial aspect of cecum2.5 cm below the ileocecal junction • Body n tip; • Rectocecal 74% • Pelvic 21% • Paracecal 2% • Subcecal 1.5% • Preileal 1% • Post ileal .5%
PERITONEAL COVERINGS • Complete • Attached to lower layer of mesentry of small intestine to form a mesntry of its own the mesoappendix
BLOOD SUPPLY • ARTERIAL • Appendicular artery a branch of lower division of ileocolic artery • An accessory appendicular artery may b present • VENOUS • Appendicular vein joins posterior cecal vein
LYMPHATIC DRAINAGE • 4,6 or more lymphatics traverse the mesoappendix to empty into ileocecal lymph nodes
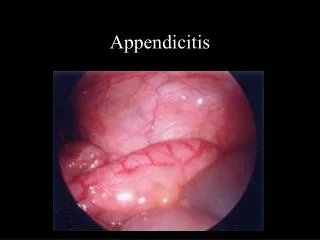
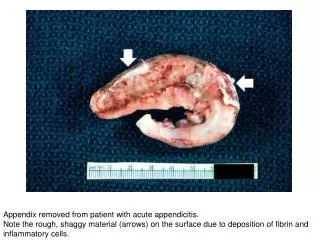
Definition • Acute inflammation of appendix • Histologically characterized by the presence of neutrophylls in the muscularis propria
ETIOLOGY • Exact etiology unknown • DIET • Rich in meat n refined CHO low in fibre • OBSTRUCTION • Of lumen by a fecolith,stricture foreign body,worms • Of the orrifice by ca cecum
PATHOGENESIS • In 50-80% of cases inflammation of the appendix is associated with obstruction • OBSTRUCTION BY A FECOLITH,GALLSTONES,BALL OF WORMS • INFLAMMATION N CONTINUOS SECRETION OF MUCINOUS FLUIDS • INC.INTALUMINAL PRESSURE • COLLAPSE OF DRAINING VEINS • STASIS N ISCHEMIA FAVOURS BACTERIAL PROLIFERATION
PATHOGENESIS Minority of inflammed appendix have no luminal obstruction and pathogenesis in such cases remain unknown
CLINICAL PRESENTATION • SYMPTOMS • Colicky abdominal pain; initially in periumbilical or epigastrium then after few hrs shift to RIF • Anorexia • Vomiting---infreqent
SIGNS • GENERAL SIGNS • FEVER 99-100 F • TACHYCARDIA 80-90 beats/min
Pointing sign • Patient is asked to point where the pain begin & where it moved
Cough sign • Ask the patient to cough will elicite tenderness in rt. Iliac fossa
McBurney sign • A sign of acute appendicitis • Deep tenderness at mcBurney point
Psoas sign • When inflammed appendix lies on psoase msl, pt. lie with rt. Hip flexed for pain relief.an attempt to hyperextend the hip will result in tenderness
Obturator sign • When hip is flexed & internally rotaded, pt. will experience pain in hypogastrium.if inflammed appendix is in contact with obturator internus
Rovsing sign • Pressure on left iliac fossa may cause pain in right iliac fossa
OUT COME OF ACUTE APPENDICITIS • RESOLUTION • ULCERATION • SUPPORATION • FIBROSIS • GANGRENE • PHLEGMONOUS MASS • APPENDICULAR ABSCESSES • MUCOCELE OF APPENDIX • GENERAL PERITONITIS
DIFFERENTIAL DIAGNOSIS • IN CHILDREN • MESENTERIC LYMPHADENITIS • MECKEL’S DIVERTICULITIS • INTUSSUCEPTION • HENOCH SCHOLEN’S PURPURA • LOBAR PNEUMONIA
D/Ds IN CHILDREN • MESENTERIC LYMPHADENITIS • Colicky abdominal pain • Cervical lymph nodes may b enlarged • MIECKEL’S DIVERTICULITIS • Colicky abdominal pain may b left sided • May b history of lower GI bleeding
DIFFERENTIAL DIAGNOSIS Henoch- scholenpurpura 1. Severe abdominal pain 2. often preceded by sore throat 3. echymotic rash on extensor surfase
Differential diagnosis in adults • Terminal ilietis • Perforated peptic ulcer • Acute pancreatitis • Rectus sheath hematoma • Testicular tortion • Rt. Side acute pyelonephritis
Differential diagnosis in adults • Rt. Side acute pyelonephritis tenderness in loin fever increased frequency of micturation • Acute pancreatitis dx by serum or urine amylase measurement
Differential diagnosis in adults females • PID • Mittelschmerz • Ectopic pregnency • Rupture ovarian cyst • Endometriosis
Differential diagnosis in adults females PID bilateral pain vaginal discharge dysmenorrhea burning pain on micturation cervical & adenexal tenderness
Differential diagnosis in adults Rupture ovariancyst pelvic U/S & gynecological opinion helpful in DX
Mittelschmerz 1. pain subside within hour 2. systemic upset is rare
Differential diagnosis in adult female Ectopic pregnency usually rt sided hx of missed menstural period positive pregnency test cervical excitation positive pelvic U/S
Differential diagnosis in elderly • Diverticulitis • Intestinal obstruction • Ceacal carcinoma • Aortic aneurism
INVESTIGATION • CBC • URINE ANALYSIS • IMAGING STUDIES • XRAY • U/S • CT • PREGNENCY TEST IN CHILD BEARING AGE
D/D’s IN ELDERLY • SIGMOID DIVERTICULITS • Abdominal CT in all pts over the age of 60 yrs • CA CECUM • Previous hx of abdominal discomfort • Alteration of bowel habits • Wt loss • Palpable mass • Barium enema is usually diagnostic
CBC moderate leukocytosis 10,000 to 16,000 Sensitivity (70 to 90%) Specificity is very low
Urine analysis • Abnormal UA result found to be in 19 to 40% • Abnormalities include pyuria hematuria & bactereuria
ABDOMINAL X RAY PLAIN ABDOMINAL XRAY localized rt. Lower quadrant ileius or radio opaque fecolith XRAY WITH BARIUM ENEMA filling defect in ceacum indicate appendicitis Abnormal findings: fecalith, appendiceal gas, localized paralytic ileus, blurred right psoas, and free air
U/S • ABDOMINAL • accuracy is 90% • PELVIC U/S • to exclude tubal or ovarian disease
U/S • Limitations of US: 1. retrocecal appendix may not be visualized 2. perforations may be missed due to return to normal diameter
CT • best choice • Greater sensitivity,98% accurate • Show • inflammed appendix • fecolith • abscess • perforation • Exclude diverticulitis & intestinal obstruction & neoplasms
Pregnancy test • Beta HCG & pelvic U/S • to exclude ectopic pregnency PID & ovarian disease