Download
1 / 50
540 likes | 933 Views
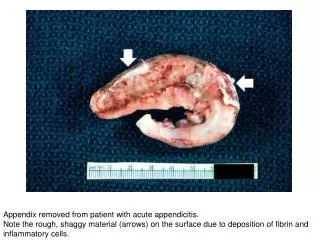
Acute Appendicitis. Dr. Mirzaei. One of the most common surgical emergencies Highest incidence in the second and third decades. Anatomy. Location: three taeniae coli converge at the base (fix) Length: <1cm to >30cm (average 6-9)

E N D
Acute Appendicitis • Dr. Mirzaei
One of the most common surgical emergencies • Highest incidence in the second and third decades
Anatomy • Location: three taeniae coli converge at the base (fix) • Length: <1cm to >30cm (average 6-9) • Tip: retrocecal, pelvic, subcecal, preileal, right pericolic
Function? • Secretion of immunoglobulin A • Appendectomy and U.C protection? • As a reservoir to recolonize the colon with healthy bacteria
Pathogenesis • Obstruction - Fecalith - Hypertrophy of lymphoid - Inspissated barium - Tumors - Vegetable and fruit - Intestinal parasites
Pathogenesis • Normal luminal capacity 0.1 ml • Proximal obstruction => closed-loop obstrucation • Normal secretion of mucosa => distention • 0.5 ml secretion => intraluminal pressure 60cm H2O
Pathogenesis • Secretion + rapid multiplication of bacteria => venous pressure increased => occlusion of capillaries • Arteriolar inflow continue => vascular congestion
Pathogenesis • Impairment of blood supply => mucosal integrity compromised => bacterial invasion • Infarction in antimesentric border => perforation
Appendiceal Rupture • Overall Rate: 25.8% • Children < 5 years: 45% • Patients > 65: 51%
Appendiceal Rupture • Walling-off process -> Phlegmon: Adherence of bowel loops to the inflamed appendix or a periappendiceal abscess. • Mass in exam:2-6% • Duration: At least 5-7 days
symptoms • Distention => visceral nerve endings stimulation => vague, dull, diffuse pain in the mid abdomen or lower epigastrium • Distention => reflex nausea &vomiting • Inflammation of serosa & parietal peritoneum => shift in pain to the right lower quadrant
Symptoms • Abdominal pain - Moderately severe - steady, sometimes intermittent cramp - 1-12 h (4-6h) pain => R.L.Q
Symptoms • Pain variation - Begins in the R.L.Q - Shift to the L.L.Q (tip in the L.L.Q) - Retrocecal => flank or back pain - Pelvic => suprapubic - Retroileal => testicular pain (irritation of the spermatic artery & ureter)
Symptoms • Intenstinalmalrotation -Visceral: normal location - Somatic: where the cecum has been arrested
Symptoms • Anorexia (nearly always) - loss of anorexia: diagnosis should be questioned
Symptoms • Vomiting - 75% of patients - neither prominent nor prolonged - only once or twice
Sequence of Symptoms • 95% anorexia – pain - vomiting • Vomiting – pain: diagnosis should be questioned
Signs • Temperature : rarely > 1ºC • PR: normal or slightly elevated • More change: complication?
Signs • Lie supine • Right thigh drawn up • Any motion increases pain • Move slowly with caution
Signs • McBurney point tenderness
Signs • Local tenderness • rebound tenderness • Voluntary guarding • True reflex (involuntary) rigidity (irritation progress)
Signs • Flank tenderness • Local tenderness in rectal exam (pelvic) • psoas sign • Obturator sign • Rovsings sign
Lab test • W.B.C 10,000 – 18,000 • Moderate P.M.N predominance • W.B.C > 18,000 => possibility of complication • CRP • U/A: several W.B.C or R.B.C (ureteral or bladder irritation) • Bacteriuria generally not seen
Imaging • Plain film (rarely helpful) - abnormal bowel gas pattern - fecalith (highly suggestive) • C.X.R (R/O right lower lobe pneumonia)
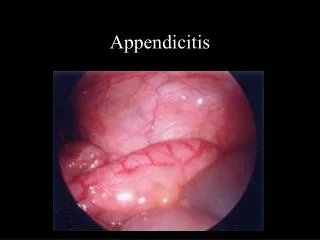
Imaging • Sonography (inexpensive, rapid, no contrast medium, even in pregnancy • Noncompressible appendix > 6mm • Appendicolith • Thickening of appendiceal wall & periappendiceal fluid • Remainder of abdominal cavity
Imaging - Sono • Exclude Gyn pathology • Effective in children & pregnancy
Imaging - sono • Limitations - user dependent - false – positive: dilated fallopian tube, inspissated stool can mimic appendicolith, obesity, - false – negative: appendicitis in tip, retrocecal, markedly enlarged, perforation
Imaging – C.T • Dilated appendix>5mm + wall thickening • thickened mesoappendix • Phlegmon • Periappendiceal fat stranding • Free fluid • Other inflammatory processes
Imaging – C.T • Expensive, exposes to radiation, cannot be used during pregnancy, allergy to contrast, intolerance of oral contast
Laparoscopy • Most useful in females (30 – 40% normal appendix) • Differentiating acute Gyn pathology
Misdiagnosis • highest rate: child-bearing women,veryyoung,very old • Accuracy of preoperative diagnosis should be: 85% • Accuracy>90%: Missed some patients • Depends on: anatomic location of the appendix, simple or ruptured, age, sex
Alvarado scale • 7-10 high likelihood • 4-6 consider further imaging • 1-3 low likelihood
Acute Mesenteric Adenitis • Most in Children • Upper respiratory tract infection is present or has recently subsided. • Pain is diffuse • Tenderness is not sharply localized • Guarding sometimes present
Acute Mesenteric Adenitis • True rigidity is rare • Generalized lymphadenopathy (may) • Relative lymphocytosis suggestive • Self limited • May need immediate exploration
Gynecologic Disorders • Pelvic Inflammatory Disease • Usually bilateral • Nausea & Vomiting: 50% • Tenderness Usually lower • Motion of cervix is painful • Diplococci on smear of purulent vaginal discharge • Higher during early phase of cycle
Gynecologic Disorders • Ruptured Graafian Follicle • Spillage of follicular fluid • Pain and tenderness diffuse • Leukocytosis & fever: minimal • Midcycle: Mittelschmerz
Gynecologic Disorders • Twisted Ovarian Cyst • Sudden pain • CT & Sono (transvaginal) • Need emergent operation • Leakage of ovarian cyst: Treated nonoperatively
Gynecologic Disorders • Ectopic pregnancy • Abnormal menses • Missing one or two periods or only slight vaginal bleeding • Elevated level of human chorionic gonadotropin(B-HCG) • Hct level falls • Vaginal exam:cervical motion tenderness • culdocentesis
Acute Gastroenteritis • Diarrhea, nausea, vomiting • Abdominal Cramps • Soft Abdomen between cramps • No localizing sign • Vomiting - Pain
Cecum or sigmoid Diverticulitis • Meckel’s Diverticulitis • Perforating Carcinoma of the cecum • Epiploicappendagitis • Pleuritis of the right lower chest • Acute Cholecystitis • Acute Pancreatitis • Hematoma of the abdominal wall • Epididymitis, Testicular torsion, U. T. I, Ureteral Stone