Download
1 / 16
160 likes | 336 Views
Theory of HFV. High Frequency Ventilation. Defined by FDA as a ventilator that delivers more than 150 breaths/min. Delivers a small tidal volume, usually less than or equal to anatomical dead space volume.

E N D
High Frequency Ventilation • Defined by FDA as a ventilator that delivers more than 150 breaths/min. • Delivers a small tidal volume, usually less than or equal to anatomical dead space volume. • While HFV’s are frequently described by their delivery method, they are usually classified by their exhalation mechanism (active or passive).
Differences between HFOV and CMV CMV HFOV Rates 0 - 150 180 - 900 Tidal Volume 4 - 20 ml/kg 0.1 - 5 ml/kg Alv Press 0 - > 50 cmH2O 0.1 - 5 cmH2O End Exp Vol Low Normalized
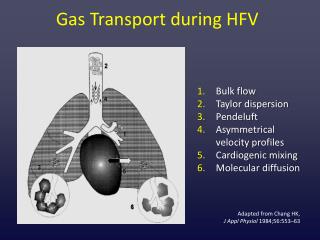
HFV Gas Exchange • Henderson first published his findings in 1915, assessing dead space relationship in ventilation. • He stated, “there may easily be a gaseous exchange sufficient to support life even when Vt is considerably less than dead space.”
HFV Gas Exchange • In the 1970’s, Bunnell and his associates demonstrated in animals that adequate alveolar ventilation could be achieved with a frequency between 5 - 30 Hz and a Vt of 20 - 25% less volume than anatomical dead space. • Slutsky, et al. theorized that the gas exchange mechanism was caused by the “coupled effects” of convection and molecular diffusion.
HFV Gas Exchange • Chang theorized that convective processes were more predominant with an increase in Vt and lower frequencies. A diffusive mechanism may be more predominant where there is a decrease in Vt and higher frequencies are used.
High Frequency Ventilation • Types of HFV’s Approved for use in both Neonates and Pediatrics • SensorMedics 3100A HFOV • Bird Volumetric Diffusive HFPPV • Types of HFV’s Approved for use in Neonates Only • Bunnell Life Pulse HFJV • Infrasonics Infant Star (discontinued) HFFI
Bunnell Life Pulse Jet • Delivers a pulse of gas into the ETT via a special adapter and pinch valve mechanism • Exhalation is Passive • Frequency of 4 - 11 Hz • Peak Airway Pressure of • 8- 50 cmH2O • Used in tandem with a • conventional ventilator • Mean Airway Pressure limited to conventional ventilator capabilities
Infrasonics Infant Star HFFI • Modification of the conventional Infant Star • Facilitated/Passive Exhalation • Pressure waveform manipulated by a series of pneumatic valves • Frequency of 2 - 22 Hz • Paw cannot be adjusted directly. Usually adjusted by changing end expiratory pressure on CMV (limited to 24 cmH2O) • Fixed 18 ms inspiratory time
Bird Volumetric Diffusive Vent • A pneumatic cartridge (Phasitron) interrupts the pressurized gas source • Passive Exhalation • Frequency of 1.6 - 21.6 Hz • Paw is not directly adjusted • May deliver HFV on top of a conventional breath
Sensor Medics 3100A • Electrically powered, electronically controlled piston-diaphragm oscillator • Paw of 3 - 45 cmH2O • Pressure Amplitude from 8 - 110 cmH2O • Frequency of 3 - 15 Hz • Inspiratory Time 30% - 50% • Flow rates from 0 - 40 LPM
3100A • “True” Oscillator • Produces an active exhalation, and does not depend on passive recoil of the chest for CO2 removal • Stand Alone Ventilator • Does not require nor deliver a conventional breath through the system • Does not require a special ET tube
3100A Ventilator • Approved in 1991 for Neonatal Application for the treatment of all forms of respiratory failure. • Approved in 1995 for Pediatric Application, with no upper “weight limit”. For treating selected patients failing conventional ventilation.
Remember • Each device has specific labeling restrictions for its use. Many devices are classified as “RESCUE ONLY” or for treating only a specific pathology. • No clinical comparisons between devices. • Each has its own indications and risks. • Strategies to treat each disease process is specific to the device used.