Download

1 / 25
270 likes | 559 Views
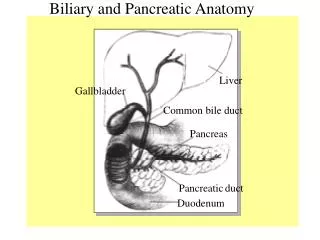
Pancreatic carcinoma and periampulary tumors. MH Emami Poursina Hakim Research Institute IUMS Isfahan, Iran 5.10 1392. Liver, Biliary System, and Pancreas. Pancreatic masses. Pancreatitis/cyst/ Pseudocyst Autoimmune pancreatitis(AP) Neuroendocrine Tumors Lymphoma

E N D
MH Emami • Poursina Hakim Research Institute • IUMS • Isfahan, Iran • 5.10 1392
Pancreatic masses • Pancreatitis/cyst/Pseudocyst • Autoimmune pancreatitis(AP) • Neuroendocrine Tumors • Lymphoma • Distal CBD cholangiocarcinoma • Pancreatic metastasis • Periampulary tumors • Exocrine pancreatic neoplasms" includes all tumors that are related to the pancreatic ductal and acinar cells and their stem cells (including pancreatoblastoma)
Epidemiology • Cancer of the exocrine pancreas is a highly lethal malignancy. • It is the fourth leading cause of cancer-related death in the United States and second only to colorectal cancer as a cause of digestive cancer-related death
Pancreatic CA risk factors • Heritage • Age • Sex • Oxidized fats • Cigarettes • Alcohol • opium • Low exercise, sedentary life • obesity • Chronic Inflammation ( pancreatitis) • Low intake of vegetable and Fibers • DM • Immunosuppressants
Surgical resection is the only potentially curative treatment. • Unfortunately, because of the late presentation, only 15 to 20 percent of patients are candidates for pancreatectomy. • Furthermore, prognosis is poor, even after a complete resection. • Five-year survival after pancreaticoduodenectomy is about 25 to 30 percent for node-negative and 10 percent for node-positive disease.
Of the several subtypes of ductaladenocarcinoma, most share a similar poor long-term prognosis, with the exception of colloid carcinomas, which have a somewhat better prognosis.
The most frequent symptoms of pancreatic CA at the time of diagnosis • Asthenia – 86 percent • Weight loss – 85 percent • Anorexia – 83 percent • Abdominal pain – 79 percent • Epigastric pain – 71 percent • Dark urine – 59 percent • Jaundice – 56 percent • Nausea – 51 percent • Back pain – 49 percent • Diarrhea- 44 percent • Vomiting – 33 percent • Steatorrhea – 25 percent • Thrombophlebitis – 3 percent
The most frequent signs of pancreatic CA at the time of diagnosis • Jaundice – 55 percent • Hepatomegaly- 39 percent • Right upper quadrant mass – 15 percent • Cachexia – 13 percent • Courvoisier’s sign (nontender but palpable distended gallbladder at the right costal margin) – 13 percent • Epigastric mass – 9 percent • Ascites – 5 percent
Signs of advanced, incurable disease include: • An abdominal mass or ascites • Left supraclavicularlymphadenopathy (Virchow's node) • A palpable periumbilical mass (Sister Mary Joseph’s node) or a palpable rectal shelf are present in some patients with widespread disease. Pancreatic cancer is the origin of a cutaneous metastasis to the umbilicus in 7 to 9 percent of cases
Clues suggesting the possibility of a primary pancreatic lymphoma include • Lack of jaundice, • Constitutional symptoms (weight loss, fever, and night sweats), • Elevated serum lactate dehydrogenase (LDH) or beta-2 microglobulin level, • Normal serum CA 19–9
An endoscopic ultrasound (EUS)-guided biopsy may be recommended if a diagnosis of chronic or autoimmune pancreatitis is suspected on the basis of history (eg, extreme young age, prolonged ethanol abuse, history of other autoimmune diseases), particularly if further imaging studies (either EUS, endoscopic retrograde cholangiopancreatography, magnetic resonance cholangiopancreatography) reveal multifocal biliary strictures (suggestive of autoimmune pancreatitis) or diffuse pancreatic ductal changes (suggestive of chronic pancreatitis).
The rates of unresectable disease among all patients with a CA 19-9 level ≥130 units/mL versus <130 units/mL were 26 and 11 percent, respectively. Among patients with tumors in the body/tail of the pancreas, more than one-third of those who had a CA 19-9 level ≥130 units/mL had unresectable disease.
The addition of molecular genetic analysis (eg, assay for K-ras or p53 gene mutations by RT-PCR) to cytologic examination may improve sensitivity, especially in patients with small primary tumors.
Screening for Extra-Colonic Cancers in Peutz-Jeghers Syndrome(2)