Download
1 / 17
180 likes | 293 Views
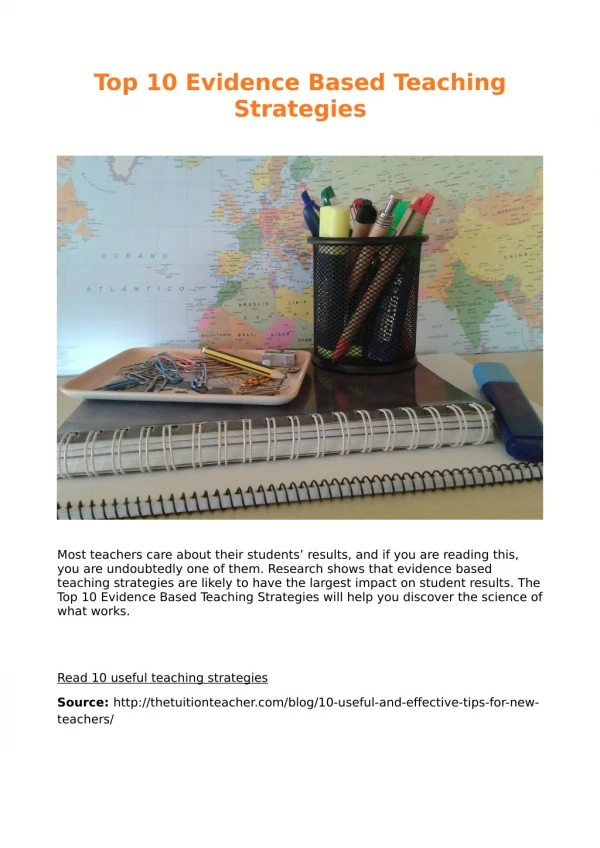
Disseminating Evidence-Based Strategies Associated With Improved Immunization Rates. Denise H. Benkel, MD, MPH Bureau of Immunization New York City Department of Health and Mental Hygiene. NICHQ. National Initiative for Children’s Healthcare Quality Not-for-Profit

E N D
Disseminating Evidence-Based Strategies Associated With Improved Immunization Rates Denise H. Benkel, MD, MPH Bureau of Immunization New York City Department of Health and Mental Hygiene
NICHQ • National Initiative for Children’s Healthcare Quality • Not-for-Profit • Partners with AAP, ABP, and IHI • Mission: To reduce the gap between what is and what could be in healthcare for all children.
NIS Results Estimated vaccination coverage among NYC children 19 to 35 months of age
Evidence-based strategies to improve immunization delivery • Parent reminders for upcoming visits and recall notices • Nurse and/or physician reminders/prompts • Parent education and expanded access to services, such as after-hours/weekends • Quality improvement efforts, including repeated measurement of immunization levels of an office practice’s one and two-year-olds • Standing orders for RN’s, PA’s, and medical assistants • Multi-component interventions
Gap between evidence and practice Much is known about how immunization delivery should be conducted, but… Knowledge of what should be done does not always translate into practice, and… There are many reasons for this gap
Improving immunization delivery in New York City • Identify evidence-based best practices • Design a strategy for effective dissemination to all NYC childhood immunization providers • Dissemination Strategy Document • toolkit • facilitated “peer-to-peer” spread • Create a relatively easy way to assess change
NICHQ Practice Assistance Approach to improvement • Steps • Performance measurement and feedback • Creation of office team and selection of goals • Testing changes • Spread of effective changes to entire practice • Tools • Clinical guidelines, academic detailing sheets • Materials tailored to office routines • Training and support (clinical and QI) • Initially, on-site visits
Phases of the project • Phase I EQuIP Collaborative:April 2002—April 2003 • Phase II Dissemination Strategy:current • Phase III Development: next • Phase IV Implementation: future
Phase I: EQuIP Collaborative • April 2002-April 2003 • Nineteen pediatric healthcare providers • 6: preventive services • 13: asthma • Successful strategies • coordination of immunization reminders with WIC visits • use of preventive services prompting sheets • telephone reminder systems • use of Citywide Immunization Registry (CIR) • enthusiasm, will, and collaboration
Phase II: Dissemination Strategy • Interviews to generate ideas • EQuIP Collaborative teams • DOHMH staff • health policymakers • Design Team • DOHMH • NICHQ • local clinical consultants
Workgroup 1: Practice Outreach and Assistance • Lessons learned from current system: QI tools must be seamless and useful • Strategies for change • patient pre-set list online Registry • bring online CIR access to large facilities • access to physicians-in-training • recall features • contact/fine non-reporters
Workgroup 2: Communication • Lessons learned from current system: There are many communication tools • Strategies for change • information and feedback should be better coordinated • key messages should be well-timed and regularly repeated • highlight common problems, while tailoring to individual provider’s needs
Workgroup 3: Measurement • Lessons learned from current system: Is difficult but extremely important • Strategies for change • special programming of Registry for regular monitoring of coverage • process and outcome measures • grouping of providers • customized reports for monitoring and feedback
Design Meeting • Public and private sectors • Managed care • Professional medical organizations • Advocacy
Phase III: Development • Customize the NICHQ toolkit to NYC • Recruit leaders and champions • Develop communication and linkages to key organizations • Build technical infrastructure • refine CIR programming • refine staffing issues
Phase IV: Implementation • DOHMH outreach staff • Site field staff • Incremental expansion • Continuous assessment of overall program performance