Download
1 / 107
1.07k likes | 1.22k Views
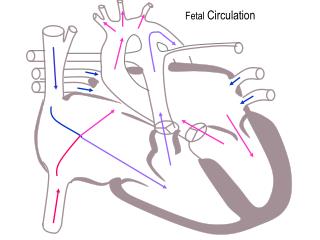
FETAL CIRCULATION. IN HEALTH AND DISEASE. Characteristics of fetal circulatory dynamics. Parallel arrangement of two main arterial systems and their respective ventricles. Mixing of venous return and preferential streaming. High impedance and low flow of pulmonary circulation.

E N D
FETAL CIRCULATION IN HEALTH AND DISEASE
Characteristics of fetal circulatory dynamics • Parallel arrangement of two main arterial systems and their respective ventricles. • Mixing of venous return and preferential streaming. • High impedance and low flow of pulmonary circulation. • Low impedance and high flow of placental circulation. • Presence of shunts.
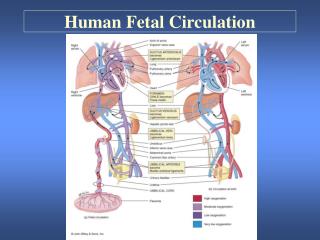
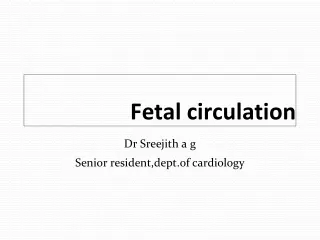
Cardiac output and its distributionFetal lamb • CVO is 450 ml/kg/wt • RV ejects 2/3 and LV ejects 1/3 of CVO • UV flow is 200 ml/mt/kg [45% of CVO] • Of this,110 ml/mt [24%] passes through DV and 90 ml/mt[21%] passes through hepatic circulation
Cardiac output and its distributionFetal lamb • Portal venous flow forms 7% and of CVO and abdominal IVC blood forms 30% of CVO. • Total venous return to heart from IVC is 315 ml/mt and represents 70% of CVO. • Of this 115 ml/mt [25% of CVO] passes through FO and and 200 ml/mt [44%] passes through TV.
Cardiac output and its distributionFetal lamb • Venous return to heart from SVC is 90 ml/mt/ and represents 21% of CVO most of this passes through tricuspid valve. • RV ejects about 300 ml/mt or about 66% of CVO. • About 35 ml/mt [8% of CVO] enters the pulmonary circulation
Cardiac output and its distributionFetal lamb • About 265 ml/mt [60%]passes through ductus arteriosus. • LV ejects 150 ml/kg [ 33% ]. • Of this,90 ml/mt [20%] distributed to head and upper half and 45 ml/mt [10%]passes through isthmus. • 3% of CVO enters coronary circulation.
60% 20% AA 33% 21% 8% 28 19 18 66% 70% 24% 24 70% 21% 32 45% 55%
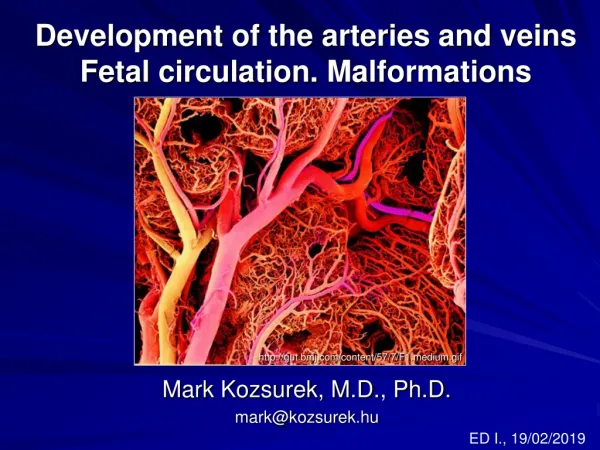
65% 65% 50% 55% 35%
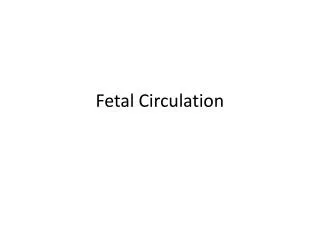
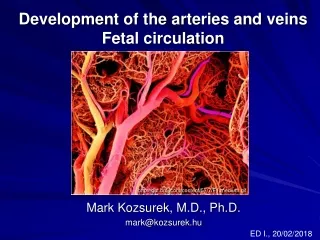
Cardiac output and its distributionhuman fetus • Limited data only is available based on doppler studies. • Umbilical blood flow is 180 ml/mt /kg of estimated fetal weight. • Pulmonary blood flow is estimated to be 75 ml/kg of fetal weight
Cardiac output and its distributionhuman fetus • CVO appears to be similar to that in lamb, 450 ml/mt/kg fetal weight • Ratio of RV output to LV output is only 1.2 to 1.3 as compared to 2:1 in fetal lamb
140 45 175 15 75 250 200 220 95 125 140 75 180 15 220 40
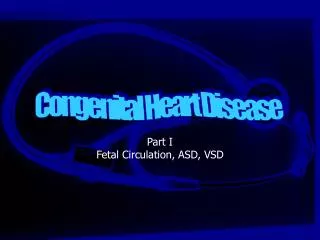
31 10 39 3 17 58 44 49 31 28 21 17 3 49 39 10
Venous return to heart • Umbilical vein gives branches to left lobe of liver and then divides into DV and arcuate vien. • Arcuate vien joins the portal vein and then gives of branches to right lobe of liver. • Left hepatic vein joins the DV at it’s entry to IVC and Right hepatic vein joins the IVC directly.
Venous return to heart • Right lobe of liver poorly oxygenated portal venous blood and left lobe receives well oxygenated umbilical venous blood. • Both lobes receive small contribution of blood from hepatic artery. • Saturation of RHV is lower than that of LHV.
Venous return to heart • Posterior and left stream of IVC blood carries oxygenated blood while anterior and right stream carries poorly oxygenated blood. • Preferential streaming of DV and LHV blood across the foramen ovale and abdominal IVC and RHV blood across the TV.
Venous return to heart • Eustechian valve helps to direct the IVC blood to cross the foramen ovale. • The lower margin of septum secundum [christa dividens] helps to direct the left posterior stream to preferentially across the foramen ovale. • SVC blood is directed aross the TV.
Shunts in fetal circulation • Ductus venosus • Foramen ovale • Ductus arteriosus or aortic isthmus
Shunts in fetal circulation • The blood returning to heart through venacavae and then redistributed to tissues without being delivered to placenta represents effective R to L shunt. • The blood which passes through DV and then reaches DA and goes to placenta without getting distributed to tissues represent effective L to R shunt. • Combined R to L and L to R shunts forms 33% of CVO.
PULMONARY CIRCULATION • Fetal lung does not serve gas exchange function. • PVR is high and PBF is low. • This helps to reduce workload of fetal heart.
PULMONARY CIRCULATION • MPA continues as Ductus and RPA and LPA arise as branches. • Medial layer is composed of smooth muscle predominantly in small pre acinar and large acinar level arteries. • Further branches have no muscular component.
PULMONARY CIRCULATION • PA pressure rises gradually paralleling the rise in aortic pressure. • TPR falls gradually but this fall when correlated with rise in lung weight, there is actually an increase in PVR towards term . • PBF increases gradually.
PULMONARY CIRCULATION • MPA has forward flow throughout systole with a short period of backflow at end of systole. • DA also has forward flow throughout systole. • BPA has forward flow only through initial one third of systole followed by back flow through rest of systole and diastole. • In humans forward flow is more prolonged.
PULMONARY CIRCULATION • Experiments show fetal PBF increases dramatically in response to increase in maternal PO2. • This response is evident only in latter part of gestation. • Doppler studies indicate similar changes in humans as well.
PULMONARY CIRCULATION • Fetal pulmonary endothelium behaves in a similar fashion as adult endothelium to vasodilators. • Adrenomedullin has a potent and prolonged vasodilatory effect. • Leukotriens may be responsible for maintaining high fetal PVR.
PULMONARY CIRCULATION • Breathing at birth is associated with a marked fall in PVR and rise in PBF. • PA pressure does not fall as rapidly and remain elevated till the Ductus is widely patent. • Once the ductus is closed, PA pressure can vary independent of systemic pressure.
Oxygen exchange function • Higher hemoglobin level in fetus as compared to mother facilitates oxygen uptake by the fetus in the placenta. • Oxygen dissociation curve of fetal red cells is shifted to left as compared to adult red cells. • HbF has less affinity towards organic phosphates like 2,3 DPG and ATP.
Oxygen exchange function • These phosphates that are present in red cells compete with oxygen for binding to hemoglobin. • Affinity of reduced hemoglobin to 2,3 DPG is higher than that of oxyhemoglobin and this facilitates oxygen delivery at tissue site. • This is not significant in fetal hemoglobin.
Oxygen exchange function • As CO2 crosses placenta from fetus to mother,it creates a local acidosis. • In the face of decreasing Ph,mothers hemoglobin shows less affinity towards Hb and oxygen release is enhanced.[Bohr effect] • This supports diffusion of more oxygen across the diffusion membrane to fetus.
Oxygen exchange function • As O2 is released,maternal Hb acts as a buffer that removes H+ from local environment. • This encourages production of bicarbonate from H2O and CO2 thereby reducing local PC02 and facilitating diffusion of CO2 from fetus.
Post natal changes • Gas exchange function is transferred from placenta to the lungs. • Separation of systemic and pulmonary circulations • Increased metabolism to maintain body temperature and hence increased cardiac output.
Post natal changes in various circulatory beds • Coronary Blood flow decreases dramatically as the oxygen content increases. • Cerebral circulation also behaves in the same fashion as coronary circulation.
Post natal changes in various circulatory beds • Skin blood flow is high in utero as the vessels are dilated because the skin is exposed to warm amniotic fluid. • Cutaneous vasoconstriction occurs post natally as evaporation from skin starts. • Cutaneous flow falls and the vascular resistance increaes.
Post natal changes in various circulatory beds • Hepatic blood flow falls rapidly post natally with reduction in umbilical venous return and then increases as the GI flow is re established. • Hepatic blood flow progressively increases after birth and by 7 days after birth reaches a level of 250 ml/minute /100 g by which time there is no flow through ductus venosus.
Changes in Cardiac output • Oxygen consumption increases from 6-8 ml/mt/kg body weight pre natally to 15 –20 ml/mt/kg post natally. • CVO of fetal lamb is 450 ml/mt/kg. • C.O of neonatal lamb is 300 -425 ml/mt/kg.So the CVO will be 600 -850 ml/mt/kg. • So the increase is 1.5 to 2 times.
Changes in Cardiac outputMechanisms • Neonate has to increase the metabolism to increase the body temperature as it is exposed to external temperature. • Improved diastolic function due to removal of compression by maternal organs and uterus causes increased cardiac filling and hence the cardiac output.
Characteristics of fetal circulatory dynamics • Parallel arrangement of two main arterial systems and their respective ventricles. • Mixing of venous return and preferential streaming. • High impedance and low flow of pulmonary circulation. • Low impedance and high flow of placental circulation. • Presence of shunts.
Cardiac output and its distributionFetal lamb • CVO is 450 ml/kg/wt • RV ejects 2/3 and LV ejects 1/3 of CVO • UV flow is 200 ml/mt/kg [45% of CVO] • Of this,110 ml/mt [24%] passes through DV and 90 ml/mt[21%] passes through hepatic circulation
Cardiac output and its distributionFetal lamb • Portal venous flow forms 7% and of CVO and abdominal IVC blood forms 30% of CVO. • Total venous return to heart from IVC is 315 ml/mt and represents 70% of CVO. • Of this 115 ml/mt [25% of CVO] passes through FO and and 200 ml/mt [44%] passes through TV.
Cardiac output and its distributionFetal lamb • Venous return to heart from SVC is 90 ml/mt/ and represents 21% of CVO most of this passes through tricuspid valve. • RV ejects about 300 ml/mt or about 66% of CVO. • About 35 ml/mt [8% of CVO] enters the pulmonary circulation
Cardiac output and its distributionFetal lamb • About 265 ml/mt [60%]passes through ductus arteriosus. • LV ejects 150 ml/kg [ 33% ]. • Of this,90 ml/mt [20%] distributed to head and upper half and 45 ml/mt [10%]passes through isthmus. • 3% of CVO enters coronary circulation.
Cardiac output and its distributionhuman fetus • Limited data only is available based on doppler studies. • Umbilical blood flow is 180 ml/mt /kg of estimated fetal weight. • Pulmonary blood flow is estimated to be 75 ml/kg of fetal weight
Cardiac output and its distributionhuman fetus • CVO appears to be similar to that in lamb, 450 ml/mt/kg fetal weight • Ratio of RV output to LV output is only 1.2 to 1.3 as compared to 2:1 in fetal lamb
Venous return to heart • Umbilical vein gives branches to left lobe of liver and then divides into DV and arcuate vien. • Arcuate vien joins the portal vein and then gives of branches to right lobe of liver. • Left hepatic vein joins the DV at it’s entry to IVC and Right hepatic vein joins the IVC directly.
Venous return to heart • Right lobe of liver poorly oxygenated portal venous blood and left lobe receives well oxygenated umbilical venous blood. • Both lobes receive small contribution of blood from hepatic artery. • Saturation of RHV is lower than that of LHV.
Venous return to heart • Posterior and left stream of IVC blood carries oxygenated blood while anterior and right stream carries poorly oxygenated blood. • Preferential streaming of DV and LHV blood across the foramen ovale and abdominal IVC and RHV blood across the TV.
Venous return to heart • Eustechian valve helps to direct the IVC blood to cross the foramen ovale. • The lower margin of septum secundum [christa dividens] helps to direct the left posterior stream to preferentially across the foramen ovale. • SVC blood is directed aross the TV.