Download
1 / 12
550 likes | 2.84k Views
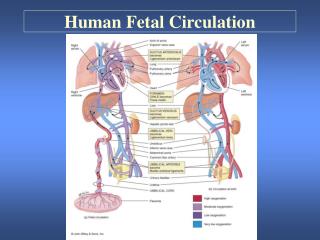
FETAL CIRCULATION. The fetal circulation is the circulatory system of a human fetus, often encompassing the entire fetoplacental circulation that also includes the umbilical cord and the blood vessels within the placenta that carry fetal blood.

E N D
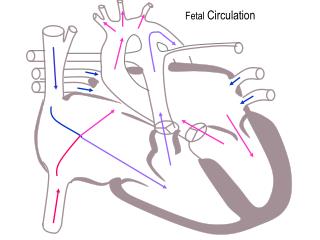
The fetal circulation is the circulatory systemof a human fetus, often encompassing the entire fetoplacental circulation that also includes the umbilical cordand the blood vessels within the placentathat carry fetal blood. The fetal circulation works differently from that of born humans, mainly because the lungs are not in use: the fetus obtains oxygen and nutrients from the mother through theplacentaand the umbilical cord. Placental role The core concept behind fetal circulation is that fetalhemoglobinhas a higher affinity for oxygen than does adult hemoglobin, which allows a diffusion of oxygen from the mother's circulatory system to the fetus. The circulatory system of the mother is not directly connected to that of the fetus, so the placenta functions as the respiratory center for the fetus as well as a site of filtration for plasma nutrients and wastes. Water, glucose, amino acids, vitamins, and inorganic salts freely diffuse across the placenta along with oxygen. The uterine arteries carry oxygenated blood to the placenta, and permeates the sponge-like material there. Oxygen then diffuses from the placenta to the chorionic villus, an alveolus-like structure, where it is then carried to the umbilical vein. At birth. At birth, when the infant breathes for the first time, there is a decrease in the resistance in the pulmonary vasculature, which causes the pressure in the left atrium to increase relative to the pressure in the right atrium. This leads to the closure of the foramen ovale, which is then referred to as the fossa ovalis. Additionally, the increase in the concentration of oxygen in the blood leads to a decrease in prostaglandins, causing closure of the ductusarteriosus. These closures prevent blood from bypassing pulmonary circulation, and therefore allow the neonate's blood to become oxygenated in the newly operational lungs.
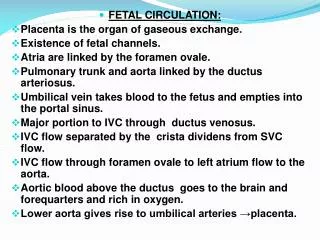
CIRCULATORY CHANGES AFTER BIRTH. Objectives.1. Review of Fetal Circulation2. Changes after Birth3. Postnatal circulation4. Defects I. Review of Fetal Circulation. The development of the cardiovascular system -� Begins to develop toward the end of the third week� Heart starts to beat at the beginning of the fourth week� The critical period of heart development is from day 20 to day 50 after fertilization.� Many critical events occur during cardiac development, and any deviation from this normal pattern can cause congenital heart defects, if development of heart doesn't occur properly. Three shunts in the fetal circulation 1. Ductusarteriosus� protects lungs against circulatory overload� allows the right ventricle to strengthen� high pulmonary vascular resistance, low pulmonary blood flow� carries mostly med oxygen saturated blood 2. Ductusvenosus� fetal blood vessel connecting the umbilical vein to the IVC� blood flow regulated via sphincter� carries mostly in oxygenated blood.
3. Foramen ovale� shunts highly oxygenated blood from right atrium to left atrium II. Review of respiratory changes and other changes at birth. Overview.� As soon as the baby is born, the foramen ovale, ductusarteriosusductusvenosus and umbilical vessels are no longer needed.� The sphincter in the ductusvenosus constricts, so that all blood entering the liver passes through the hepatic sinusoids.� Occlusion of the placental circulation causes an immediate fall of blood pressure in the IVC and right atrium. Circulatory Adjustments after birth: Increasing uptake of oxygen by lungs (first and subsequent breaths) induces a vasoconstriction of ductusvenosus and ductusarteriosis Aeration of the lungs at birth is associated with:1. a dramatic fall in pulmonary vascular resistance due to lung expansion.2. a marked increase in pulmonary blood flow (thus raising the left atrial pressure above that of IVC)3. a progressive thinning of the walls of the pulmonary arteries (due to stretching as lungs increase in size with first few breaths) The first breath: � the pulmonary alveoli opens up:� pressure in the pulmonary tissues decreases� Blood from the right heart rushes to fill the alveolar capillaries� Pressure in the right side of the heart decreases� Pressure in the left side of the heart increases.
Resulting circulatory changes include:� blood pressure is now high in the aorta and systemic circulation is well established Control of circulation is a reflex function regulated:� Peripherally by the baroreceptors in the aortic artch and carotid sinus� Centrally by baroreceptors in the cardiovascular center of the medulla (in close proximity of the chemoreceptors that regulate respiration)� Respiratory and circulatory reflexes are usually strong in the healthy full-term newborn, but their efficiency in controlling cardiovascular function is susceptible to environmental factors. Foramen ovale� Before birth the foramen ovale allows most of the oxygenated blood entering the right atrium from the IVC to pass into the left atrium� Prevents passage of blood in the opposite direction because the septum primum closes against the relatively rigid septum secundum.� Closes at birth due to decreased flow from placenta and IVC to hold open foramen,and� More importantly because of increased pulmonary blood flow and pulmonary venous return to left heart causing the pressure in the left atrium to be higher than in the right atrium.� The increased left atrial pressure then closes the foramen ovale against the septum segundum.� The output from the right ventricle now flows entirely into the pulmonary circulation.
Other changes in the heart.� The right ventricular wall is thicker than the left ventricular wall in fetuses and newborn infants because the right ventricle has been working harder. By the end of the first month the left ventricular wall is thicker than the right because it is now working harder than the right one. The right ventricular wall becomes thinner because of atrophy associated with its lighter workload. DuctusArteriosus,� The DA constricts at birth, but there is often a small shunt of blood from the aorta to the left pulmonary artery for a few days in a healthy, full-term infant.� In premature infants and in those with persistent hypoxia the DA may remain open for much longer.� Oxygen is the most important factor in controlling closure of the DA in full-term infants. Closure of the DA appears to be mediated by bradykinin, a substance released by the lungs upon initial inflation.� Bradykinin has potent contractile effects on smooth muscle. Action depends upon the high oxygen content of the aortic blood resulting from aeration of the lungs at birth.� When the PO2 of blood passing through the DA reaches about 50 mm Hg, the wall of the DA constricts. (May be mediated direct or may be mediated by Oxygen's effect on decreasing PG E2 and prostacylcin secretion. (unlike in a coarctation of aorta which requires PGE2 infusion to reopen the DA for blood flow.� As a result of reduced pulmonary vascular resistance, the pulmonary arterial pressure falls below the systemic level and the blood flow thru the ductusarteriosis is diminished.
Umbilical Arteries constrict at birth� To prevent loss of infant's blood.� Umbilical cord is not tied for 30-60 seconds so that blood flow thru umbilical vein continues, transferring fetal blood from placenta to the infant.� Blood change from fetal to adult pattern of circulation is not a sudden occurrence in some changes occur during the first breath, others over hours and days. Adult Derivatives of Fetal Vascular Structures� Because of certain changes in the cardiovascular system at birth, certain vessels and structures are no longer required.� Over a period of months these fetal vessels form nonfunctional ligaments, and fetal structures such as the foramen ovale persist as anatomic vestiges of the prenatal circulatory system. Adult Derivatives of Fetal Vascular Structures� Because of certain changes in the cardiovascular system at birth, certain vessels and structures are no longer required.� Over a period of months these fetal vessels form nonfunctional ligaments, and fetal structures such as the foramen ovale persist as anatomic vestiges of the prenatal circulatory system.
CONGENITAL HEART DEFECTS. 1.Left to right shunt: ventricular septal defect Arterial septal defect patent ductusarteriosus 2.Right to left shunt: Tetralogy of fallot Pulmonary atresia Transposition of the great arteries Total anomalous pulmonary venous drainage 3.Obsructive: Aortic stenosis Pulmonary stenosis Coarctation of the aorta Hypoplastic left heart Three common defects: 1.patent ductusarteriosus(acyanotic)� common in females 2-3 times more than males, unknown reason why� Most common congenital anomaly associated with maternal rubella infection during early pregnancy (mode of action by virus unclear)� Premature infants usually have a PDA due to hypoxia and immaturity.� Surgical closure of PDA is achieved by ligation and division of the DA. Characterisedby:increased pulmonary blood flow,increased ascending aorta volume,increased left arterial and left ventricle volume.
CLINICAL SYMPTOMS FOR PDA • Delay of physical development • dyspnea,fatiguability,paleness,Often respiratory diseases • widening of heart borders to upper and left • systolic “purr of cat” • 2. Patent foramen ovale� most common form of an Atrial Septal Defects (ASDs)� a small isolated patent foramen ovale is of no hemodynamic significance; but if other defects present (e.g. pulmonary stenosis or atresia), blood is shunted through the foramen ovale into the left ventricle, producing cyanosis, a dark bluish coloration of the skin and mucous membranes resulting from deficient oxygenation of the blood.� A probe patent foramen ovale is present in up to 25% of people. A probe can be passed from one atrium to the other through the superior part of the floor of the fossa ovalis. Though not clinically significant (usually small)but may be forced open because of other cardiac defects and contribute to functional pathology of the heart. Results from incomplete adhesion between the original flap of the valve of the foramen ovale and the septum secundum after birth. • CLINICAL SYMPTOMS FOR ASD. • Widening of heart border to the right • fatigueability,dyspnoe,systolicmurmur,present at age >1
3.Ventricular septal defect(VSD) • They are most frequent congenital anomally.This defect is usually acyanotic because the greater pressure in the left ventricle causes a shunt from left to right. • CLINICAL SYMPTOMS OF VSD • Delay of physical development • Deformation of the chest(cardiac humpback) • Systolic “purr of cat”(vibration) • dyspnea,weakness,fatiguability,pallor,heart failure • In percussion,all heart borders are expanded • Infective endocarditis • X ray shows cardiomegaly • Frequent respiratory diseases.
COMPLICATIONS. • Congestive heart failure.This serious complication, which makes it difficult for the heart to pump blood to the body, usually develops in the first six months after birth in babies who have a significant heart defect. Signs of congestive heart failure include rapid breathing, often with gasping breaths, and poor weight gain. • Slower growth and development.Children with congenital heart defects often develop and grow more slowly than do children who don't have heart defects. Your child may be smaller than other children of the same age and, if the nervous system has been affected, may learn to walk and talk later than other children. • Pneumonia.Having a congenital heart defect makes your child more prone to respiratory tract infections, including pneumonia. • Heart rhythm problems,paleness,respiratory disorders, systolic “purr of cat” , dyspnea,weakness,fatiguability. • Cyanosis.If your child's heart defect causes oxygen-rich and oxygen-poor blood to mix in his or her heart, your child may develop a grayish-blue skin color, a condition called cyanosis. • Stroke.Although uncommon, some children with congenital heart defects are at increased risk of stroke due to blood clots traveling through a hole in the heart and on to the brain. • Emotional issues.Some children with congenital heart defects may feel insecure or develop emotional problems because of their size, activity restrictions or learning difficulties. Talk to your child's doctor if you're concerned about your child's moods.
TREATMENTS AND DRUGS. Procedures using catheters:Some children and adults now have their congenital heart defects repaired using catheterization techniques, which allow the repair to be done without surgically opening the chest and heart. In procedures that can be done using catheterization, the doctor inserts a thin tube (catheter) into a leg vein and guides it to the heart with the help of X-ray images. Once the catheter is positioned at the site of the defect, tiny tools are threaded through the catheter to the heart to repair the defect. Open-heart surgery:In some cases, your child's doctor won't be able to fix your child's heart defect using a catheter procedure. In these cases, your child's doctor may perform open-heart surgery to try to repair your child's heart defect. These surgeries are major medical procedures and may require a long recovery time for your child. Heart transplant:if a serious heart defect can't be repaired, a heart transplant may be an option. Medications:Some mild congenital heart defects, especially those found later in childhood or adulthood, can be treated with medications that help the heart work more efficiently.e.g Antiplatelet and antiarrhytmic drugs...