Download
1 / 11
120 likes | 360 Views
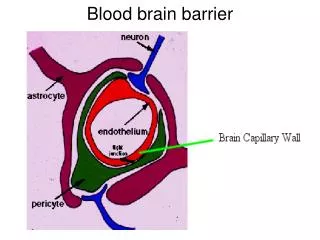
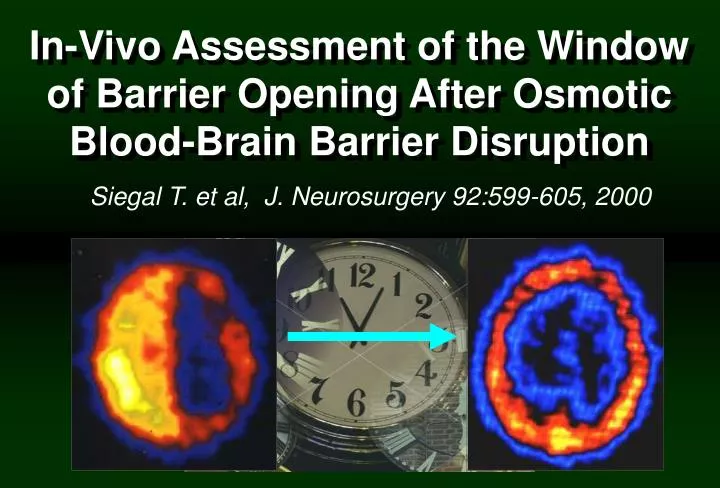
In-Vivo Assessment of the Window of Barrier Opening After Osmotic Blood-Brain Barrier Disruption. Siegal T. et al, J. Neurosurgery 92:599-605, 2000. TcGH SPECT after BBBD. 1 min. 90 min. 240 min. 480 min. Siegal T et al: J Neurosurgery 92:599-605, 2000. BBBD and PCNSL.

E N D
In-Vivo Assessment of the Window of Barrier Opening After Osmotic Blood-Brain Barrier Disruption Siegal T. et al, J. Neurosurgery 92:599-605, 2000
TcGH SPECT after BBBD 1 min 90 min 240 min 480 min
BBBD and PCNSL • At present osmotic BBBD is employed in a multicenter setup. • The results of a phase II study (OHSU) has been published. • With the marked increase in drug penetration and prolonged period of incompletely restored barrier function - neurotoxicity is the major concern. • Safety profile:Complication rate across different centers is similar (Doolittle et al. Cancer 88:637-47, 2000).
Adverse Effects Procedure Related Adverse Events: • Treatment related death – 1/474 (0.2%) • Minor strokes – 2/474 (0.4%) • Arterial injuries successfullyrepaired by stenting – 2/474 (0.4%) • Reversible brainstem lesioninduced by carboplatin – 1/474 (0.2%) • Seizures – 38/474 (8%) Events/Procedures
McAllister et al: Neurosurgery 46:51-61, 2000 PCNSL: SurvivalBBBD + Chemotherapy, No RT n= 74 Median: 40.7 mo 5-year survival: 42% Siegal T. et al: Neuro-Oncol 7(3):312, 2005 N=33 Median survival : 40 mo 5-year survival: 41%
Time to Tumor Progression PFS: 24 mos – 69% 36 mos – 57% Siegal T. et al: Neuro-Oncol 7(3):312, 2005
SURVIVAL and PFS:(Multicenter Study-HD-MTX Based Combination ChemoTx + XRT) DeAngelis LM et al:JCO 20:4643-8, 2002
Follow-Up: Cognitive Function • Median follow-up is 27mos (range:5-94 ) • 19/33 (58%) patients are being followed for more than 24 months • Of patients followed for > 24 mos none demonstrated delayed leukoencephalopathy • No progressive cognitive loss was observed on clinical and neuropsychological testing.
Mean Neuropsychological Score Indices in Patients > 60 y.o. Treated with BBBD Chemotherapy and No RT McAllister et al: Neurosurgery 46:51-61, 2000