Download
1 / 48
530 likes | 1.05k Views
Complex Coronary Cases. Supported by: Abbott Vascular Boston Scientific Corporation Medtronic, Inc. Astrazeneca. Disclosures. Samin K. Sharma, MBBS, FACC Speaker’s Bureau – Boston Scientific Corporation, Abbott, The Medicines Company, Daiichi Sankyo, Inc. and Lilly USA, LLC

E N D
Complex Coronary Cases Supported by: Abbott Vascular Boston Scientific Corporation Medtronic, Inc. Astrazeneca
Disclosures Samin K. Sharma, MBBS, FACC Speaker’s Bureau – Boston Scientific Corporation, Abbott, The Medicines Company, Daiichi Sankyo, Inc. and Lilly USA, LLC Annapoorna S. Kini, MBBS, FACC Nothing to disclose Sameer Mehta, MBBS, FACC Consulting Fees – The Medicines Company American College of Cardiology Foundation staff involved with this case have nothing to disclose
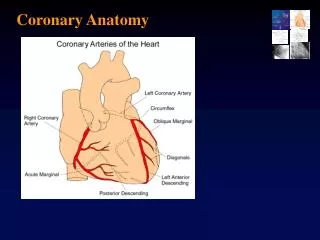
March 19th 2013 Case #9: CS, 73 yr M Presentation: Presented on 2/8/2013 with cresendo CCS class III angina & exertional dyspnea. Pt had stress MPI revealing severe anterior and lateral ischemia. Echo in past revealed severe MR and minimal LV dysfunction; surgical repair recommended but declined. Cath revealed 3 V CAD and LVEF 55%. SYNTAX score 25. Cardiac surgery recommended but again declined after Heart-Team discussion. Pt underwent Xience Xpedition DES to LCx-HL and prox LAD and did well. Pt Still has residual class II angina. Prior History: Hyperlipidemia, Hypertension, H/o CVA Medications: All once daily dosage Aspirin 81mg, Clopidogrel 75mg, Metoprolol XL 100mg, Diltiazem CD 180mg, Rosuvastatin 20mg
Case# 9: cont… SYNTAX score 25 Cardiac Cath 2/8/2013: Left Dominance 3 Vessel CAD with LVEF 56% Left Main: Mild diffuse disease LAD: 80-90% lesion in prox, total D1 fills via collaterals LCx: 90% distal LCx with 80% OM1 bifurcation lesion Ramus Intermedius: 95% lesion, moderate size PCI: Underwent Xience Xpedition DES (3/23mm) to pLAD and Xience Xpedition DES (2.5/28mm) to Ramus Intermedius Plan Today: - PCI of bifurcation lesion of circumflex (SYNTAX score 16)
Issues Involving The Case • Two DES for bifurcation lesions • Newer devices for calcified lesions
Issues Involving The Case • Two DES for bifurcation lesions • Newer devices for calcified lesions
Coronary Artery Bifurcation Lesion Interventional Techniques Interventional Bifurcation Techniques One Stent Technique (OST) Crush Stent Technique (CrST) Kissing Stent Technique (SKS) ‘T’ Stent Technique (TST) OST with SBR Dilatation (SBT) Culotte Stent Technique (CUT)
12.8 11.4 4.5 2.1 Clinical Outcomes in Trials Comparing One-DES (1S) vs. Two-DES (2S) Strategy in Treating Coronary Bifurcations MACE TLR 19 18.0 15.8 15.2 15 13.6 12.9 11.9 % 12.0 10.9 8.0 9.5 8.0 8.9 7.2 5.8 5.6 5.6 3.4 4.5 2.9 4.0 1.9 1.0 1S 2S 1S 2S 2S 1S 2S 1S 2S 1S 2S 1S 2S 1S Colombo et al. CACTUS trial (n=85) Ferenc et al. T-stenting (n=202) Steigen et al. NORDIC Trial (n=413) Pan et al. SES stents (n=91) Colombo et al. SES stents (n=85) Sharma et al. PRECISE-SKS (n=100) Hildick et al. BBC ONE (n=500)
Clinical Outcomes in Trials Comparing One-DES (1S) vs. Two-DES (2S) Strategy in Treating Coronary Bifurcations Incidence of Reported Stent Thrombosis 1S group 2S group 3.5 3.0 3.0 % 2.0 2.0 1.7 1.1 0.5 0.4 0 0 0 0 0 1S 2S 2S 1S 2S 2S 1S 2S 1S 2S 1S 2S 1S 1S Colombo et al. SES stents (n=85) Steigen et al. NORDIC Trial (n=413) Colombo et al. CACTUS trial (n=85) Ferenc et al. T-stenting (n=202) Hildick et al. BBC ONE (n=500) Sharma et al. PRECISE-SKS (n=100) Pan et al. SES stents (n=91)
DKCRUSH Technique for Bifurcation Lesions 1. SBr stenting 2. Balloon crush 3. 1st Kissing balloon inflation 4. MV stent and crush 5. Final Kissing balloon inflation Chen S et al. J Interven Cardiol 2009;22:127
A Randomized Clinical Study Comparing Double Kissing Crush With Provisional Stenting for Treatment of Coronary Bifurcation Lesions: DK Crush II Study Conventional (n= 185) p<0.001 % DK Crush (n=185) 22.2 p=0.017 p=0.07 17.3 14.6 p=0.036 10.3 9.7 p=0.37 6.5 4.9 3.8 2.2 0.5 ST Main Vessel Side Vessel MACE TVR Angiographic Restenosis Chen S et al, JACC 2011;57:914
DK-CRUSH III Study Flowchart of Study Design Chen et al., JACC 2013 In Press
DK-CRUSH III Study TVR-Free Survival Rate at 12 M MACE-Free Survival Rate at 12 M Chen et al., JACC 2013 In Press
DK-CRUSH III Study: Clinical F/U at 12 Months DK Group (N = 210) p=0.001 Culotte Group (N = 209) p=0.03 % p=0.38 p=1.00 p=0.62 Chen et al., JACC 2013 In Press
DK-CRUSH III Study Forest Plots of 1-Year MACE Rate in Pre-Specifies Subgroups Chen et al., JACC 2013 In Press
BBC One Study: 9-Month Post-PCI Scores on SAQ for Simple and Complex Groups Sirker et al., JACC Cardiovasc Interv 2013;6:139
BBC One Study: Direction of Change in Individual Patients’ Scores on SAQ Sirker et al., JACC Cardiovasc Interv 2013;6:139
Issues Involving The Case • Two DES for bifurcation lesions • Newer devices for calcified lesions
Facts about Calcified Lesions Angiography underestimates the presence, extent and axial depth of calcium Calcium significantly increases procedural complications Most studies have excluded calcified lesions While rotational atherectomy (RA) allows for greater stent expansion, studies have reported increased late loss and restenosis, likely due to platelet activation and thermal injury from the device Thus, at the present time, RA is mainly reserved for undilatable or extremely calcified lesions. Mintz et al., Circ 1995;01:1959, Lofberg et al., Cardiovasc Interv Radiol 1998;19:317, Davies et al., J Am Coll Surg 2005;201:275, Gallino et al., Circ 1984;70:619, Becquemin et al., J Endovasc Surg, 1995;2:42, Zdanowski et al., Int Angio 1999;18:251, Vroegindeweij et al., Cardiovasc Interv Radiol 1997;20:420
Impact of Severity of Coronary Calcification on 1-Year Outcomes After PCI in NSTEMI/STEMI: Insight from an angiographic pooled analysis from ACUITY and HORIZONS Trials Généreux, TCT 2012
Frequency of Moderate/Severe Calcification in ACS Population n = 6,855 patients Moderate/Severe None/Mild Généreux, TCT 2012
1-Year Ischemic Outcomes: ACS Population (N= 6855 patients) p=0.001 None/Mild Moderate/Severe p=0.002 % p=0.22 p=0.0002 p=0.001 p=0.007 Généreux, TCT 2012
Device Selection for Various Coronary Lesions Type * All Comers/Fibrotic Undilatable/Mild-Mod Calcified Heavily Calcified AngioSculpt Compliant or Non-compliant Balloon
Balloon Atherotomy Cutting Balloon (Flextome) • - Security & performance are engineered to: • Reduce vessel wall expansion • Maximize plaque compression • Relief hoop stress • - Better results with lower inflation pressure • compared to plain old balloon angioplasty Longitudinal microtomes Indications: -Mild calcified -Inelastic/chronic -Ostial -ISR AngioSculpt balloon
Post-procedure Stent Luminal Area ≥5.0 mm2 p=<0.001 % Costa et al., Am J Cardiol 2007;100:812
Stent Expansion by Plaque Morphology % Optimal Stent Expansion Costa et al., Am J Cardiol 2007;100:812
ROTAXUS 240 patients with calcified lesions enrolled between August 2006 and March 2010 at 3 clinical sites in Germany 1:1 randomization Mean age 71 DM 28% MVD 74% Ostial 18% Bifurc 48% B2/C 90% IVUS not used Rotoblator + PES (n=120) PTCA + PES (n=120) - 2 patients died in-hospital - 6 patients withdrew consent - 5 patients lost at follow-up Clinical follow-up at 9 months in 96.2% (n=227) Angio follow-up at 9 months in 80.5% (n=190) *Primary endpoint: In-stent late loss Richert, TCT 2011
ROTAXUS: 9-month Follow-up p=0.46 ROTA + PES (n=123) PTCA + PES (n=132) p=0.73 % p=0.84 p=0.79 p=0.78 p=1.0 * Defined as death, MI and TVR Richert, TCT 2011
ORBITAL ATHERECTOMY: Unique Mechanism of Action Differential Orbital Sanding Crown will only sand the hard components of plaque Soft components (plaque/tissue) flex away from crown • Orbital Mechanism • Increased speed = Increased centrifugal force • Greater centrifugal force = Larger orbital diameter CF=Mass X Rotational speed2 Radius of the orbit
Orbital Atherectomy Technology for Calcified Coronary Arteries • Easy setup and use • Control of device in operating field • .012” OAS guide wire • Compatible with 6 French guiding catheters
ORBITAL Atherectomy: Unique Mechanism of Action • Orbiting Crown Enables • Continous flow of blood and saline • Minimizes thermal injury • Potentially decreases no-reflow and periprocedural cardiac enzyme elevation • One crown treats different vessel diameters based on orbiting speed
The Differences Between Sanding and Drilling Bi-directional Uni-directional
ORBIT I Trial • First-in-man study using orbital atherectomy in coronary arteries • Designed to demonstrate safety and performance in calcified coronary lesions • Prospective, single-arm • 2 centers OUS • 50 subjects with >90⁰ of calcium via IVUS • Compared to ORBIT II • Shorter lesions • Less B2/C lesions • Parikh et al., Catheter Cardiovasc Interv 2012, March 5 • 2. Parikh et al., JACC Cardiovasc Interv 2013;6:Suppl 5
ORBIT II Study Design • To evaluate safety and efficacy of coronary OAS to prepare de novo severely calcified coronary lesions for enabling stent placement • Prospective • Multi-center trial • Single arm – FDA recommendation as there are no FDA-approved percutaneous treatments for patients with severely calcified lesions. 443 patients enrolled in 49 US sites 30 days follow-up Complete in 97.7 % (N=430/443) Chambers, ACC 2013
ORBIT II Study Design • Primary Safety Endpoint: 30-Day MACE • Cardiac death • MI defined as CK-MB level > 3 times upper limit of lab normal (ULN) value • With or without abnormal Q-wave • Target vessel revascularization (TVR) • Primary Efficacy Endpoint: Procedural Success • Success in facilitating stent delivery with a final residual stenosis of <50% and without in-hospital MACE Chambers, TCT 2012
The ORBIT II Trial: An Historic Coronary Study ORBIT II Study Unique Study Design to Evaluate Higher Risk CAD Patients SEVERELY CALCIFIED ARTERIES DIALYSIS PATIENTS INCLUDED EF < 35% INCLUDED Chambers, TCT 2012
The ORBIT II Trial: Primary Safety Endpoint 30 Day MACE Rate Components: MI (CK-MB >3x ULN): 9.7% Non Q-wave 8.8% Q-wave 0.9% TVR/TLR: 1.4% TVR 0.7% TLR 0.7% Cardiac death: 0.2% Freedom from 30 Day MACE = 89.8% Performance Goal = 83% 95% CI = 87.0%, 92.7% 80% 85% 90% 95% 100% Chambers, ACC 2013
The ORBIT II Trial: Primary Efficacy Endpoint Procedural Success Components: Successful Stent Delivery: 97.7% Less than 50% residual stenosis: 98.6% In-hospital MACE: 9.5% MI (CK-MB >3x ULN)/TVR/TLR: 9.3% Non- Q-wave 8.6% Q-wave 0.7% TVR 0.7% Cardiac death: 0.2% Procedural Success = 89.1% Performance Goal = 82% 95% CI = 85.8%, 91.8% 80% 85% 90% 95% 100% Chambers, ACC 2013
The ORBIT II Trial: 30 Day Results (N=443) Patients with Severely Calcified Coronary Lesions Underwent Diamondback 360⁰ Orbital Atherectomy at 49 States Primary Efficacy Endpoint of Procedural Success Primary Safety Endpoint of Freedom from MACE % % Successful <50% In-hospital MI TVR Cardiac stent residual MACE death delivery stenosis Chambers, ACC 2013
Take Home Message:Two stent strategy and devices for calcified lesions • Appropriately done 2 stent treatment strategy is emerging as the superior strategy over 1 stent in large coronary bifurcation lesions. Hence no longer the issue should 1 or 2 DES; rather we should identify lesions which will need 2 DES and plan accordingly (rather then bailout strategy) • Orbital atherectomy system in heavily calcified coronary lesions appears very promising and once available, has a chance for wider acceptance because of effectiveness and simple setup and easy learning curve.
Question # 1 • DK-Crush technique has shown to be superior to other stent strategy for bifurcation lesions except : • Lower restenosis • Lower TVR • Lower MACE • Lower stent thrombosis
Question # 2 • Orbital atherectomy trials have shown 9-12M MACE rate of: • 6-10% • 11-15% • 16-20% • 21-25% • E. >25%
Question # 3 • Statement about mechanism of Orbital atherectomy is true: • A. Lumen gain is proportional to the size of the burr • B. Lumen gain is proportional to burr movement • C. Lumen gain is proportional to the burr speed
Question # 1 • DK-Crush technique has shown to be superior to other stent strategy for bifurcation lesions except : • Lower restenosis • Lower TVR • Lower MACE • Lower stent thrombosis The correct answer is D. While DK Crush trials have shown lower MACE and restenosis, thee has been no difference in the incidence of stent thrombosis.
Question # 2 • Orbital atherectomy trials have shown 9-12M MACE rate of: • 6-10% • 11-15% • 16-20% • 21-25% • E. >25% The correct answer is A. Both ORBIT I and II trials showed MACE rate of <10% at 1 year follow-up. All was largely due to small non-Q wave MI.
Question # 3 • Statement about mechanism of Orbital atherectomy is true: • A. Lumen gain is proportional to the size of the burr • B. Lumen gain is proportional to burr movement • C. Lumen gain is proportional to the burr speed The correct answer is C. Lumen gain after Orbital atherectomy is dependent on the burr speed; faster it is, more arc it covers and larger is the lumen gain.