Download
1 / 51
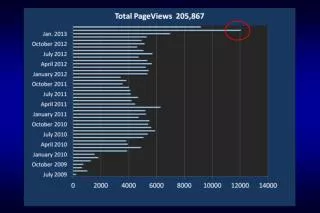
660 likes | 1.39k Views
Frailty, Complex Cases in Geriatrics. Min H. Huang, PT, PhD, NCS. Learning Objectives. Define frailty from Fried model and dynamic frailty model Explain the measurement of frailty in older adults Adapt physical therapy management for frail, complex geriatric clients

E N D
Frailty, Complex Cases in Geriatrics Min H. Huang, PT, PhD, NCS
Learning Objectives • Define frailty from Fried model and dynamic frailty model • Explain the measurement of frailty in older adults • Adapt physical therapy management for frail, complex geriatric clients • Utilize Modified Physical Performance Test to measure frailty for geriatric clients
Reading Assignments • Guccione 2012 Chapter 9, Chapter 26
Frailty • NOT a disease or a characterization that differentiate disability or old age • A combination of a variety of medical problems or conditions • A biological syndrome of decreased reserve and resistance to stressors • Resulting from cumulative declines across multiple physiological systems • Cause vulnerability to adverse outcomes
Frailty • Cognitive impairment should be included in the definition of frailty • cognitive impairment was associated with chronic disability, long-term nursing home stay, and death • Frailty is associated with cardiovascular disease, low education and poverty, hospitalization, institutionalization, death, increased risk for falls, deteriorating mobility, and disability.
Association of brain pathology with the progression of frailty in older adults • The accumulation of common brain pathologies contributes to progressive physical frailty in old age • The presence of macroinfarcts, Alzheimer disease, Lewybody pathology, and nigral neuronal loss was associated with a more rapid progression of frailty (all p values ≤0.010) Buchman 2013. Neurology. 2013 May 28;80(22):2055-61.
A chronic inflammation process, impaired immunity, neuroendocrine dysregulations and metabolic alterations seem to be related to frailty but true comprehension of the involved pathway is still lacking
Traditional Definition of Frailty: Fried Model • Frail: a person meets > 3 of the criteria • Prefrail: a person meets 1 or 2 of the criteria Fried 2001
Criteria used to define frailty in Fried model • Weight loss: loss > 10 lb unintentionally in the past year • Exhaustion: CES-D Depression scale (self-report question) • Physical activity: men < 383 Kcals; women < 270 Kcals • Walk time: time to walk 15 ft stratified by gender and height • Grip strength Fried 2001
Relationships between frailty, comorbidity, and disability (Fried 2001) Comorbidity: >2 diseases
Frailty Defined by Deficit Accumulation: Dynamic Model • Instruments to measure frailty have been developed based on the recent concepts of frailty as a result of cumulative deficits • Frailty instruments are mainly developed as risk assessment tools, i.e. prognostic instruments, NOT as outcome measures • Instruments typically consider multiple factors that are associated with frailty. N.M. de Vries et al. / Ageing Research Reviews 10 (2011) 104–114 105
Dynamic concepts of frailty measured by Frailty Index • Score based on the accumulation of deficits • Number of health deficits (symptoms, signs, disabilities, laboratory, radiographic) out of a list of possible deficits • Use a continuous scoring system • Thereby can discriminate and measure change after an intervention • Can capture the dynamic nature of frailty • A cut-off value for frailty has not been NOT specified
Frailty Index- Comprehensive Geriatric Assessment (FI-CGA)
The number of deficits is important: more deficits increased risk of an adverse health outcome more risk of frailty more frail Rockwood & Mitnitski 2011
PT to prevent functional decline in physically frail, elderly person (Gill 2002) • n=188; 75+ y.o. physically frail elderly living at home • 6 month home based program • Intervention: PT focusing on improving balance, strength, transfer and mobility • Control: an educational program • Intervention group had significantly less functional decline (8 ADLs) over time (up to 12 months) than control group. • Effect was seen among elderly with moderate frailty but NOT those with severe frailty
PT to prevent functional decline in physically frail, elderly person (Gill 2002)
PT to prevent functional decline in physically frail, elderly person (Gill 2002)
Physical and performance measures to identify mild to moderate frailty • Brown et al (2000) studied the correlation of physical measures (UE and LE strength, ROM, balance, coordination, sensation, and gait) with a 36-point Modified Physical Performance Test (Modified PPT) • Physical measures correlated with PPT • Frailty according to the PPT score • NOT frail = 32-36 • Mildly frail = 25-31 • Moderately frail = 17-24
Comprehensive Geriatric Assessment (CGA) • Multidimensional, multidisciplinary diagnostic instrument • Usually coordinated by a case manager • Used to collect data on the medical, psychological, functional capabilities and limitations of complex elderly patients. • To develop a coordinated and integrated plan for treatment and follow-up, including primary care and rehabilitation, and make the best use of health care resources.
Comprehensive Geriatric Assessment (CGA) • CGA focuses on • Elderly individuals with complex problems • Functional status and QoL • Frequently takes advantage of an interdisciplinary team of providers • The "Five I's of Geriatrics“ are easily missed in a standard medical evaluation • intellectual impairment, immobility, instability, incontinence and iatrogenic disorders • http://ocw.tufts.edu/data/42/499797.pdf
Benefits from the utilization of CGA • Provide diagnostic and prognostic indicators • Reduce length of hospital stay and readmission • Predict survival and detect tolerance for chemotherapy in older cancer survivors • Reduce the prevalence of orthostatic hypotension • Identify elderly patients at risk for mortality, post-discharge institutionalization, adverse in-hospital events, and prolonged length of hospital stay with pre-operative CGA
Components of the CGA • MMSE or Mini Cog for cognition • Geriatric Depression • ADL scale (Katz Index) • Physical Performance Test (PPT) • Vulnerable Elders-13 survey (VE-13) • Barthel Index (BI) • Pain Scale • Nutritional assessment • Functional assessment • Gait assessment (various tools used)
PT consideration for frail elderly • Evaluation: thorough including PMH, lab values, meds, social hx, nutritional status • Goal creation: modified as needed depending on level of illness/disability • Falls in SNFs 3x the rate of community dwellers • Fall risks: history of falls, weakness (1° quads), balance deficit, gait deficits (slowed walking speed), presence of ophthalmic disease, also a change in living conditions in the past 2 years J Blackwood
Comparison of Causes of Falls in Nursing Home and Community-Living Populations Ranked by Prevalence
Case 1 • 71-year-old female, widowed, lives alone in a 2-story home 3 steps to enter/ B/B on 1st floor • PMH: osteoarthritis, CHF with an ejection fraction of 30%, COPD, bladder incontinence, hypothyroidism, gout, osteoporosis, non-insulin-dependent diabetes mellitus, and a history of a left distal femur fracture in 2007. • PSH: CABG x4 in 2001, lumbar laminectomy (L3-L5)in 1998, and pacemaker implantation six months ago. J Blackwood
Case 1 (continued) • Meds: acetaminophen Flexeril, digoxin, Lasix, Levothyroxine, nitroglycerin, Zoloft, Coumadin, Cipro, and Zocor • HPI: The patient fell onto her right side 1 week ago at home while going outside to retrieve the mail and was hospitalized for three days for dehydration and a UTI. All x-rays were negative for fracture. • PT eval and treat in her home.
Systems review: mental status • Common causes of mental status change • hypoxemia, anemia, hyperglycemia, electrolyte imbalances, malnutrition, dehydration, and polypharmacy • Delibrium vs. dementia • Can coexist. • Delirium is a typically acute onset of inattention, disorganized thinking, a change in the level of consciousness, disorientation, decreased memory, perceptual disturbances, and altered sleep–wake cycles.
Systems review: vital signs • HR regularity: < 6 interruptions in the rhythm in 1 minute • Normal pulse pressure= 40 mmHg (e.g. resting BP = 120/80 mmHg, 120-80 = 40) • OH: a drop in systolic BP by 20 mmHg after standing 2-3 min from supine, or a drop by 10 mmHg with a reflexive increase in HR with transitional movements, e.g. supine-to-sit or sit-to-stand • Response to exertion, pulmonary function
Systems review: OH • Causes: adverse effects of drugs, anemia, dehydration, arrhythmias, immobility, sepsis, adrenal insufficiency, ANS dysfunction due to DM, Parkinson's CNS impairments • Patients may or may not have symptoms and thereby it is difficult to use symptoms as an indicator • PT must screen the patient's BP with position changes to rule out orthostatic hypotension • Patients with OH are at risk for sustaining injuries, including falls, fractures, and MI
Systems review • Senses: vision, hearing • Bowel/bladder continence • Detective work • Nutrition and body composition • Tests: ROM, strength, aerobic capacity, self-care activities, various outcomes measures (Berg, Tinetti, TUG) • Gait speed: 0.4-0.5 m/sec in institutionalized elders
Tests and measures • Choose ones that reject or confirm a hypothesis • ‘Correct’ tests and measures are ones that provide data that allow the PT to make a plausible inference about the patient’s condition. • Used to clarify the extent of a functional limitation or disability
Test of muscle strength • Limitations of MMT • NOT a quantitative assessment tool • LACK accuracy due to its severe ceiling effect • Does NOT correlate with functional tasks on certain patients • Some patients with cognitive impairments, ROM, or mobility limitations have problems with MMT • Functional testing for muscle strength: • If a patient is able to stand up from a chair without the use of his or her arms, it is safe to assume that strength on the quadriceps is at least 4
MRC (Medical Research Council) sum score • Quantify global muscle strength • 3 muscle groups in UE (shoulder abduction, wrist extension, grip strength) • 3 muscle groups in LE (hip flexion, knee extension, ankle dorsiflexion) • Score between 0 (no muscle movement) and 5 (normal strength) for each muscle group • A maximum total score of 60 • Reliable and valid too for critically ill patients • Severe weakness score < 36 • Significant weakness <48
Evaluation • Purpose • To indicate which deficiencies in function are present • To identify the impairments most associated with the current level of function and which may be remediated • Consider quality of data, likelihood of error, and the risk to the patient when evaluating the meaning of the data
ICU acquired weakness • Minimal criteria for diagnosing ICU-acquired weakness = 1, 2, 3 or 4, 5 • “Generalized weakness developing after the onset of critical illness • Weakness is diffuse (involving both proximal and distal muscles), symmetric, flaccid, and generally spares cranial nerves • MRC sum score <48 or mean MRC score, 4 in all testable muscle groups noted on <2 occasions separated >24 hours • Dependence on mechanical ventilation • Cause of weakness not related to the underlying critical illness has been excluded
Diagnostic criteria of UTI in nursing home residents • Nursing home residents without a catheter • 3+: (1) a fever > 100.4°F or greater (2) new or change in burning of urination, frequency, or urgency (3) new flank or suprapubic pain (4) change in color, consistency, or cloudiness of urine (5) change in mental or functional status. • Nursing home residents with catheters • 2+: (1) fever as noted earlier (2) new flank or suprapubic pain (3) change in presence of urine (4) change in mentation or functional status
Dehydration • Account for nearly 40% of all hospitalization admissions in older adults. • Older adults are susceptible to dehydration because • a blunted thirst mechanism • a reduction in total body fluidwith the reduction in muscle mass and an increase in body fat • a decrease in renal function that concentrates the urine prevents the body from retaining enough fluid to avert dehydration. • comorbidities
Type of dehydration • Hypertonic dehydration • Water loss > Sodium loss • Common in presence of infection or exposure to hot environmental temperatures • Isotonic dehydration • Water loss = Sodium loss • vomiting and diarrhea • Hypotonic dehydration (*Most common type) • Water loss < Sodium loss • Use of diuretics (e.g. Diuril, Lasix)