Download
1 / 1
10 likes | 83 Views
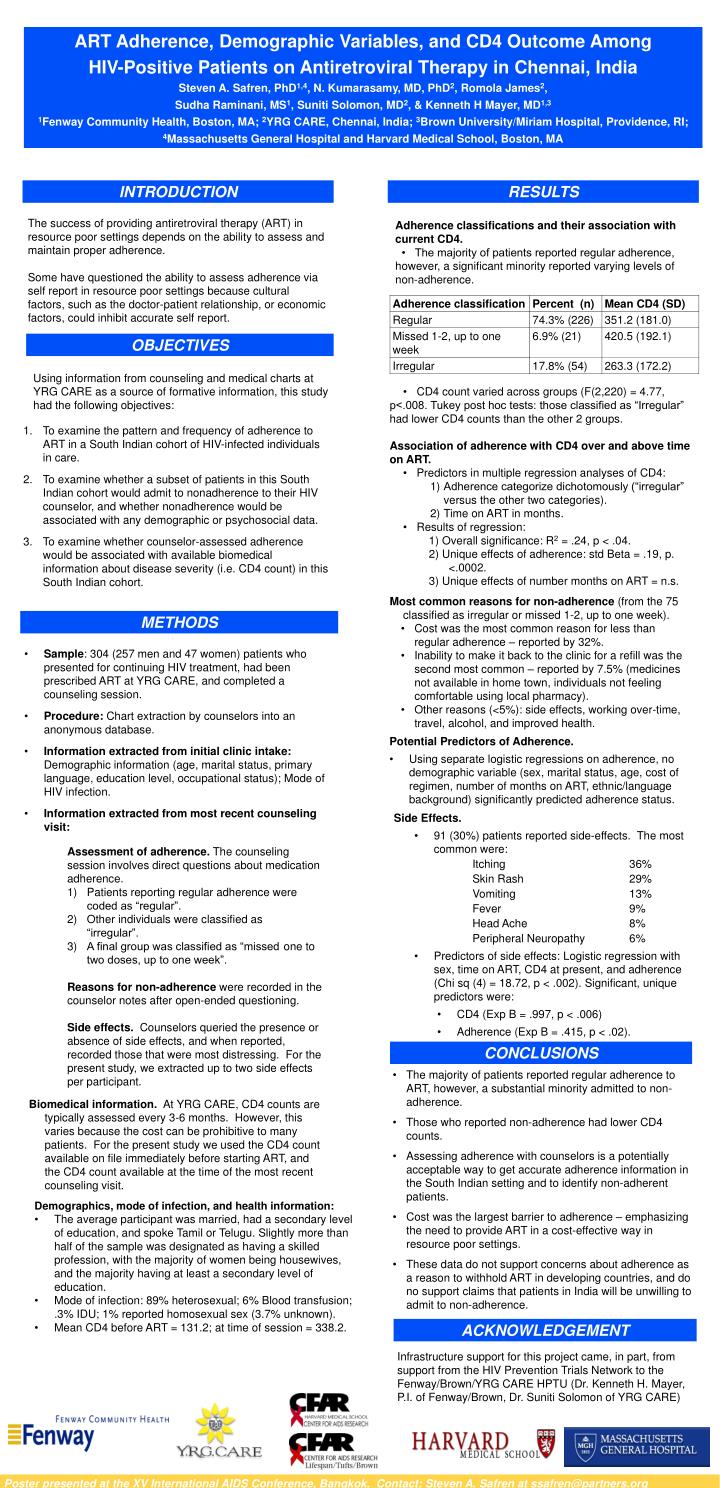
ART Adherence, Demographic Variables, and CD4 Outcome Among HIV-Positive Patients on Antiretroviral Therapy in Chennai, India Steven A. Safren, PhD 1,4 , N. Kumarasamy, MD, PhD 2 , Romola James 2 , Sudha Raminani, MS 1 , Suniti Solomon, MD 2 , & Kenneth H Mayer, MD 1,3

E N D
ART Adherence, Demographic Variables, and CD4 Outcome Among HIV-Positive Patients on Antiretroviral Therapy in Chennai, India Steven A. Safren, PhD1,4, N. Kumarasamy, MD, PhD2, Romola James2, Sudha Raminani, MS1, Suniti Solomon, MD2, & Kenneth H Mayer, MD1,3 1Fenway Community Health, Boston, MA; 2YRG CARE, Chennai, India; 3Brown University/Miriam Hospital, Providence, RI; 4Massachusetts General Hospital and Harvard Medical School, Boston, MA INTRODUCTION RESULTS The success of providing antiretroviral therapy (ART) in resource poor settings depends on the ability to assess and maintain proper adherence. Some have questioned the ability to assess adherence via self report in resource poor settings because cultural factors, such as the doctor-patient relationship, or economic factors, could inhibit accurate self report. Adherence classifications and their association with current CD4. • The majority of patients reported regular adherence, however, a significant minority reported varying levels of non-adherence. OBJECTIVES Using information from counseling and medical charts at YRG CARE as a source of formative information, this study had the following objectives: • CD4 count varied across groups (F(2,220) = 4.77, • p<.008. Tukey post hoc tests: those classified as “Irregular” • had lower CD4 counts than the other 2 groups. • Association of adherence with CD4 over and above time • on ART. • Predictors in multiple regression analyses of CD4: • Adherence categorize dichotomously (“irregular” versus the other two categories). • Time on ART in months. • Results of regression: • 1) Overall significance: R2 = .24, p < .04. • 2) Unique effects of adherence: std Beta = .19, p. <.0002. • 3) Unique effects of number months on ART = n.s. • Most common reasons for non-adherence (from the 75 classified as irregular or missed 1-2, up to one week). • To examine the pattern and frequency of adherence to ART in a South Indian cohort of HIV-infected individuals in care. • To examine whether a subset of patients in this South Indian cohort would admit to nonadherence to their HIV counselor, and whether nonadherence would be associated with any demographic or psychosocial data. • To examine whether counselor-assessed adherence would be associated with available biomedical information about disease severity (i.e. CD4 count) in this South Indian cohort. • Cost was the most common reason for less than regular adherence – reported by 32%. • Inability to make it back to the clinic for a refill was the second most common – reported by 7.5% (medicines not available in home town, individuals not feeling comfortable using local pharmacy). • Other reasons (<5%): side effects, working over-time, travel, alcohol, and improved health. METHODS • Sample: 304 (257 men and 47 women) patients who presented for continuing HIV treatment, had been prescribed ART at YRG CARE, and completed a counseling session. • Procedure: Chart extraction by counselors into an anonymous database. • Information extracted from initial clinic intake: Demographic information (age, marital status, primary language, education level, occupational status); Mode of HIV infection. • Information extracted from most recent counseling visit: • Potential Predictors of Adherence. • Using separate logistic regressions on adherence, no demographic variable (sex, marital status, age, cost of regimen, number of months on ART, ethnic/language background) significantly predicted adherence status. • Side Effects. • 91 (30%) patients reported side-effects. The most common were: • Itching 36% • Skin Rash 29% • Vomiting 13% • Fever 9% • Head Ache 8% • Peripheral Neuropathy 6% • Predictors of side effects: Logistic regression with sex, time on ART, CD4 at present, and adherence (Chi sq (4) = 18.72, p < .002). Significant, unique predictors were: • CD4 (Exp B = .997, p < .006) • Adherence (Exp B = .415, p < .02). • Assessment of adherence. The counseling session involves direct questions about medication adherence. • Patients reporting regular adherence were coded as “regular”. • Other individuals were classified as “irregular”. • A final group was classified as “missed one to two doses, up to one week”. • Reasons for non-adherence were recorded in the counselor notes after open-ended questioning. • Side effects. Counselors queried the presence or absence of side effects, and when reported, recorded those that were most distressing. For the present study, we extracted up to two side effects per participant. CONCLUSIONS • The majority of patients reported regular adherence to ART, however, a substantial minority admitted to non- adherence. • Those who reported non-adherence had lower CD4 counts. • Assessing adherence with counselors is a potentially acceptable way to get accurate adherence information in the South Indian setting and to identify non-adherent patients. • Cost was the largest barrier to adherence – emphasizing the need to provide ART in a cost-effective way in resource poor settings. • These data do not support concerns about adherence as a reason to withhold ART in developing countries, and do no support claims that patients in India will be unwilling to admit to non-adherence. Biomedical information. At YRG CARE, CD4 counts are typically assessed every 3-6 months. However, this varies because the cost can be prohibitive to many patients. For the present study we used the CD4 count available on file immediately before starting ART, and the CD4 count available at the time of the most recent counseling visit. • Demographics, mode of infection, and health information: • The average participant was married, had a secondary level of education, and spoke Tamil or Telugu. Slightly more than half of the sample was designated as having a skilled profession, with the majority of women being housewives, and the majority having at least a secondary level of education. • Mode of infection: 89% heterosexual; 6% Blood transfusion; .3% IDU; 1% reported homosexual sex (3.7% unknown). • Mean CD4 before ART = 131.2; at time of session = 338.2. ACKNOWLEDGEMENT Infrastructure support for this project came, in part, from support from the HIV Prevention Trials Network to the Fenway/Brown/YRG CARE HPTU (Dr. Kenneth H. Mayer, P.I. of Fenway/Brown, Dr. Suniti Solomon of YRG CARE) Poster presented at the XV International AIDS Conference, Bangkok. Contact: Steven A. Safren at ssafren@partners.org