Download
1 / 23
240 likes | 424 Views
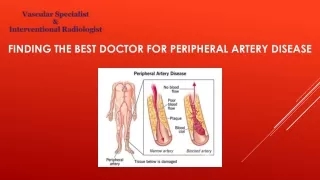
Peripheral Artery Disease of the lower extremities. Dr Asso Amin (MRCP-UK). Anatomy. Abdominal Aorta divides to 2 Common Iliac arteries at L4 Common iliac artery divides to external and internal iliac arteries

E N D
Peripheral Artery Disease of the lower extremities Dr Asso Amin (MRCP-UK)
Anatomy • Abdominal Aorta divides to 2 Common Iliac arteries at L4 • Common iliac artery divides to external and internal iliac arteries • External Iliac artery passes downwards on the medial aspect of psoas muscle to the inguinal ligaments. • As it enters the thigh it becomes the common femoral artery • Divides into superficial and deep iliac artery • Superficial femoral artery passes on the medial aspect of the femur in middle third of thigh • Enters the adductor canal and becomes the popliteal artery after it exits the inferior aspect of the canal • Anterior tibial and posterior tibial
Pathophysiology Atheroslerotic lesion. Non Atherosclerotic causes of PAD • Acute arterial disease • vasospam • radiation • takayasu’s disease • Buergers disease • fibromasculardysplesia • compartment syndrome
Epidemiology • PAD is defined as an ABPI of less than 0.90 in either leg . • 10% , raising to 15-20% over the age of 70. affects 27 Million people in Europe and North America. • NHANES ,PAD presents in 0.9% aged 40-49 , and 15% above 70 . • PARTNERS , 7000 patients over 70 or 50-69 with DM or current smoker. • PAD has 6 fold increase risk of death from CVD than without PAD
Major risk factors :- • Age ,sex and ethnicity • Smoking .Edinburgh Artery Study • Diabetes meta-analysis of 13 studies found that 1% increase of Hb1ac increase risk of PAD by 26% . Also faster progression and 10 times more likely to need major amputation. • Hypertension and Hyperlipidaemia . Framingham Heart Study 5. CKD
Clinical Presentation • A symptomatic :- • Progression to other stages • less than 20% PAD reports typical features • The role of treatment. • Claudication • Critical Limb Ischemia –Chronic • Acute Limb Ischemia
Diagnostic Evaluation • Physical examination • Ankle Brachial Index and Toe brachial Index • Normal values 0.9-1.3 • Mild Obstruction 0.7-0.9 • Moderate Obstruction 0.5-0.7 • Severe Obstruction <0.5 • ABI threshold of 0.9 has 95% sensitivity and 100% specificity • False positive in non compressible vessels ,should be suspected when ABPI is more than 1.3 or systolic BP lower is higher by 20mmHg or 20% • Non compressible vessel expected in DM, and CKD
Diagnostic Evaluation • Segmental Pressure Measurements • Continuous wave Doppler • Treadmill Exercise Testing with ABI • Vascular treadmill testing –less intense( Gardner –Skinner Bruce Control or Hiatt protocols) • ECG at same time • Symptoms or protocol completion limited • After completion –supine position and record at 1 min interval • Alternative 6 min walk or paedal plantar flexion test .
Diagnostic Evaluation • Duplex USS • Sensitivity 90% , specificity 95% • Computed Tomographic Angiogram (CTA) • location and stenosis severity. • MRA • Contrast Angiogram
Screening for a symptomatic patients • patient age above 70 years • patient between 50-70 and CVD risk factors • patient below 50 with diabetes& CVD risk factors • Screening is done by symptoms and ABI
Critical Limb Ischemia Evaluation • Conformation of diagnosis • Localizing the lesion • Assessment for need for revascularization • Assessment for operative risk ( Lee’s Revised operative risk assessment) • History and examination • Hematological and Biochemical • Hb1AC%,Lipid,GUE • Ankle/Toe pressure index • Lower limb vascular imaging • Duplex scan of carotid artery ( high risk) • Coronary assessment
Management • Supervised exercise programs • Cilostazol:- Phosphodiesterase enzyme inhibitor that increase C-Amp . • Has antiplatelets and vasodilator effect • Seven RCT ( improve walking distance by 40-60%) ,100mg BD • SE headache, flushing, dizziness, CI :- HF • Anti-platelets :- • Antithrombotic trialists meta analysis on 135000 patients , shows reduction of vascular death by 22% • Reduce risk of PAD progression • CHARISMA STUDY
Management • Anti-Hypertensive • Improve endothelial function and CVD mortality • Ramipril reduce risk of CVD in PAD by 25% . Recommended for both symptomatic and a symptomatic • ?? B- blockers • Lipid Lowering agent- • Traget LDL of less than 130mg/dl , • Treatment of DM • Smoking cessation • L-Carnitine – 2 multicentre study ,700 patients , improve walking distance
Surgical Management • Pre-operative risk assessment and Risk reduction.( Goldmans and Destky&Lee Revised risk)