Download
1 / 30
400 likes | 1.31k Views
Congenital Syphilis December 10, 2010. Renata Dennis, RN, MPH Southeast AIDS Training and Education Center (SEATEC) Emory University School of Medicine Atlanta, GA 30322. Disclosure.

E N D
Congenital Syphilis December 10, 2010 Renata Dennis, RN, MPH Southeast AIDS Training and Education Center (SEATEC) Emory University School of Medicine Atlanta, GA 30322
Disclosure • “I have no real or perceived vested interests that relate to this presentation nor do I have any relationships with pharmaceutical companies, biomedical device manufacturers, and/or other corporations whose products or services are related to pertinent therapeutic areas.” Renata Dennis, RN, MPH, 10 December 2010
Objective By the end of this session, participants will be able to: • Describe the clinical manifestations of congenital syphilis • Discuss maternal and infant testing for congenital syphilis • Describe a prevention plan for congenital syphilis
CDC Fact Sheet, updated December 2007 How common are STDS in pregnant women in the United States? Estimated Number of STDs Pregnant Women Bacterial Vaginosis 1, 080,000 Herpes Simplex virus 2 880,000 Trichomoniasis 124,000 Chlamydia 100,000 Gonorrhea 13,200 Hepatitis B 16,000 HIV 6,400 Syphilis <1,000
Tolan, R., Infectious Diseases in Clinical Practice, 01/2008 *TORCH Infections in Pregnancy T-Toxoplasmosis O-Other Infections (HIV, Hepatitis B, Syphilis, etc.) R-Rubella C-Cytomegalovirus H-Herpes Simplex *Also known as STORCH or TORCHeS (to account for the importance of Syphilis), plus other acronyms to emphasize a variety of important infections.
AETC National Resource Center, Treating Opportunistic Infection Among HIV-Infected Children, 12/2004 STD Fact Sheet, www.cdc.gov/std/Syphilis/STDFact-Syphilis.htm, downloaded 12/2010 Congenital Syphilis: Epidemiology and Pathogenesis • Perinatal transmission of Treponema pallidum at any stage of pregnancy or during delivery from an infected woman to her offspring • Drug use during pregnancy increases risk of maternal and congenital syphilis • Syphilis chancres make it easier to transmit and acquire HIV infection sexually, and • Rate of congenital syphilis 50 times greater among infants born to HIV-infected mothers
CDC Syphilis Surveillance Report, 2006; S. Philip, Congenital Syphilis, 9/2002 Congenital Syphilis: Epidemiology and Pathogenesis, cont’d. • The spirochete crosses the placenta and infects the fetus; may also occur from contact with an infectious lesion canal during delivery • In utero sonographic findings include: hydrops, thickened placenta, hepatomegaly, ascites • Any woman delivering stillbirth after 20 weeks gestation should be evaluated for syphilis
Farella, C. What if....? Pondering Clinical Cliffhangers, Nursing Spectrum, 2002 Case(s) of Congenital Syphilis ???? Henry VIII, King of England, 1491-1547 • Much controversy among historians • Wives had many miscarriages and stillbirths • The king himself had evidence of a skin disease at 22, series of headaches at 37, open leg ulcers that did not heal at 44, deformity (?gummata) on right side of nose at 45, and then, there was that temper later in life • NO WAY TO KNOW without testing-- syphilis mimics other conditions
Maranich, TORCH Infections, downloaded 12/2010 S. Philip, Congenital Syphilis, 9/2002 Congenital Syphilis:Clinical Symptoms and Manifestations Three major classifications: • Fetal effects • Early effects • Late effects Damage to fetus/infant depends on the stage of development atwhich the infection has taken place and time elapsed before treatment.
AETC National Resource Center, Treating Opportunistic Infection Among HIV Infected Children, 12/2004; A. Aaranich, Torch Infections, downloaded 12/2010 Fetal effects(prenatal/perinatal period) • Miscarriage • Stillbirth • Neonatal death Intrauterine and/or perinatal death in 25-40% of cases
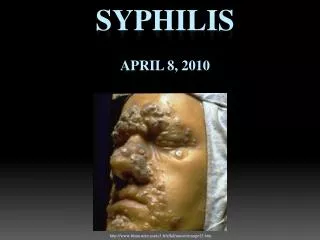
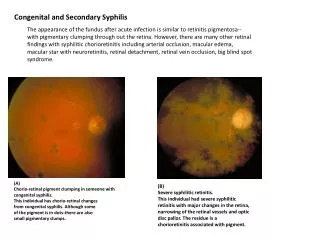
Hepatosplenomegaly- diffuse inflammation, scarring, jaundice Generalized lymphadenopathy –epitrochclear nodes Coombs – hemolytic anemia, thromobocytopenia, leukopenia, leukocytosis Hydrops fetalis Mucocutaneous: rhinitis (highly infectious), “snuffles”, mucous patches Maculopapular rash Desquamation Pemphigus syphiliticus (vesicular bullous eruptions of palms and soles) Petechial lesions Bony lesions, osteochondritis, periostitis, pseudoparalysis Syphilitc leptomeningitis Chorioretinitis, salt and pepper fundus, glaucoma Pancreatitis S.Philip, Congenital Syphilis, 9/2002 Maranich, TORCH Infections, downloaded 12/2010 AETC National Resource Center, Treating Opportunistic Infection Among HIV-Children, 1/2004 Early effects- in up to 60% of infants(usually evident within first 5 weeks, can take up to 2 years) Early manifestations are varied, with multi-system involvement
S. Philip, Congenital Syphilis, 9/2002 Papulosquamos Plaques
S. Philip, Congenital Syphilis, 9/2002 Broken vesicles, desquamation Condylomata around anus Infiltration, desquamation and rhinitis
Rhinitis (snuffles), mucous patches, damage to palate(late) S.Philip, Congenital Syphilis, 9/2002 Bullae and vesicular rash on soles Eroded papular lesions
S. Philip, Congenital Syphilis, 9/2002 Osteochondritis of distal radius and ulna Osteochondritis of femur and tibia metaphysis
Remember: • Infants may be asymptomatic at birth • And without early antibiotic treatment, children may develop: • Brain damage • Blindness • Hearing impairment • Bone and tooth abnormalities CDC STD Treatment Guidelines 2006
Interstitial keratitis (inflammatory) Nerve deafness Clutton’s Joints (synositis, restricted movement) Hutchinson’s triad (teeth, intersitial keratitis, 8th nerve deafness) Mulberry molars Flaring scapulas Hydrocephalus Mental retardation Frontal bossing, saddle nose, protruding mandible High arched palate Perioral fissures Higouemenaki’s sign(periosteal rotation of clavicle, sternocleidomastoid) Saber shins Rhagades (linear scars that become fissured or ulcerated) S. Philip, Congenital Syphilis, 9/2002 Results primarily from chronic inflammation of bone, teeth,and CNS. Late effects (manifestations after 2 years of age)
S. Philip, Congenital Syphilis, 9/2002 Hutchinson’s teeth – peg shaped upper incisors Frontal Bossing
S. Philip, Congenital Syphilis, 9/2002 Saber shins: Anterior bowing of tibias Gumma: Thin atrophic scar
AETC National Resource Center, Treating Opportunistic Infection Among HIV-Infected Children, 12/2004 Maranich, TORCH Infections, downloaded 12/2010 CDC 2006 STD Treatment Guidelines, downloaded 12/2010 Diagnosis in newborns, (difficult because of maternal antibodies) • Confirmed if organism identified in skin lesions • Presumptive, if present: physical exam findings CSF findings (positive VDRL) Osteitis on long bone x-rays Funisitis (“barber shop pole” umbilical cord) Positive IgM antibody (test is hard to get done) • Regardless of physical findings, if mother was un-or inadequately treated for syphilis
AETC National Resource Center, Treating Opportunistic Infection Among HIV-Infected Children, 12/2004 CDC 2006 Sexually Transmitted Diseases Treatment Guidelines, downloaded 12/2010 Diagnosis in newborns, cont’d. • Use combination of physical, radiologic, serologic, and direct microscopic (darkfield microscopy, flourescent antibody test of a sample)results, as standard serologic tests detect only IgG • All infants born to mothers with reactive nontreponemal and treponemal test should be evaluated with a quantitative nontreponemal test, e.g., slide test, rapid plasma reagin (RPR)
S. Philip, Congenital Syphilis, 9/2002 • If infant’s titer higher than mother’s congenital infection • If decreasing titer in infant passive transfer of antibodies, should disappear by 3-4 months of age. • Persistently reactive VDRL, with rising titer active infection • Remember: • A sustained 4-fold decrease in titer of nontreponemal test after treatment indicates adequate therapy • A 4-fold titer increase after treatment suggests re-infection or relapse. Diagnosis in newborns, cont’d.
S. Philip, Congenital Syphilis, 9/2002 Syphilis Diagnosis: A Review • Serologic tests are the principal means for diagnosis: • Nontreponemal test: VDRL, RPR • Treponemal tests: TPI, FTA-ABS, MHA-TP
S. Philip, Congenital Syphilis, 9/2002 Testing for Syphilisswitching tests can cause confusing (VDRL versus RPR)—use the same test to compare and track progress Nontreponemal: VDRL, RPR Treponemal: TPI, FTA-Abs, MHA-TP • Quantitative results correlate with disease activity, therefore, this is a helpful screening test; these tests are sensitive, but not specific • Titers rise when disease is active, fall when treatment is adequate • In congenital infection, these tests become non-reactive within a few months of adequate treatment • Used as a confirmatory test • Treponemal antibody titers become positive soon after initial infection and usually remain positive for life, even with adequate therapy • Antibody titers do not correlate with disease activity, and are not quantified
CDC 2006 STD Treatment Guidelines Treatment for Congenital Syphilis (Dependent upon clinical scenario) • Aqueous crystalline penicillin G: 100,000-150,000 units/kg/day, administered as 50 units/kg/dose IV every 12 hours during the first 7 days of life and every 8 hours thereafter for 10 days OR • Procaine penicillin G: 50,000 units/kg/dose IM in a single daily dose for 10 days OR • Benzathine penicillin G: 50,000 units/kg/dose IM in a single dose • Dosage varies for older infants and children • Other drugs are an option if there is a penicillin allergy (although desensitization may be possible) If >1 day of therapy is missed, the entire course should be restarted
S. Philip, Congenital Syphilis, 9/2002 Close follow-up of infants: • Should have careful follow-up examination at , 2, 4, 6, and 12 months of age. • Serologic non-treponemal tests: 3, 6, 12 months, and end of treatment • (or until non-reactive) • Non-treponemal Ab titers decline by 3 months of age, and should be non-reactive by 6 months, if infant was not infected. (Transplacentally acquired antibodies.) • If persistent, stable titers, consider retreatment. • Congenital neurosyphilis- CSF exam at 6 month intervals until normal.
Some questions for you: • When does your agency test pregnant women for syphilis? Is one time per pregnancy enough? • When do you treat pregnant women? Does this change if she has HIV? • Do you ask about a history of syphilis on intake? Remember: some people don’t realize you can be re-infected.
CDC 2006 STD Treatment Guidelines A Final Word (from the CDC): “No infant or mother should leave the hospital unless the maternal serologic status has been documented at least once during pregnancy, and at delivery in communities and populations in which the risk for congenital syphilis is high.” Added editorial note: The same goes for HIV.
CDC MMWR STD Guidelines, 2006* http://www.cdc.gov/std/treatment/2006/congenital-syphilis.htm http://www.cdc.gov/std/treatment/2006/n5511.pdf *New guidelines are expected any day!