Download
1 / 73
790 likes | 976 Views
Congenital Syphilis. N.Frewan, PL2 Neonatology Division July 2008. Background. Between 1905 -1910, Schaudinn & Hoffman identified T pallidum as the cause of syphilis

E N D
Congenital Syphilis N.Frewan, PL2 Neonatology Division July 2008
Background • Between 1905 -1910, Schaudinn & Hoffman identified T pallidum as the cause of syphilis • The name "syphilis" was coined by Italian physician and poet Girolamo Fracastoro in his Latin written poem “Syphilis sive morbus gallicus” ("Syphilis or The French Disease") in1530
Introduction • Curable STD caused by the Treponema pallidum organism • 1998: Complete genetic sequence of T. pallidum was published which helped understanding the pathogenesis of syphilis • Belongs to “Spirochaetaceae family” • The genus name, Treponema, is derived from the Greek term for "turning thread“
Treponema Pallidum • Thin • Motile • Extremely fastidious • Survive only briefly outside host • Not cultivated successfully on artificial media
Transmission • Direct sexual contact with ulcerative lesions of skin or mucous membranes • Trans placental: • Typically during second half of pregnancy • As early as 6 weeks of gestation • Pregnant with primary or secondary syphilis are more likely to transmit the disease than those with latent (not clinically apparent) disease Cannot be spread through contact with toilet seats, doorknobs, swimming pools, hot tubs, bathtubs, shared clothing, or eating utensils
Congenital syphilis • Severe, disabling, and often life-threatening infection seen in infants • About half of all infected fetuses die shortly before or after birth
IncidenceUS • Despite the fact of being curable if caught early, rising rates among pregnant ♀ in the US have recently ↑ the number of infants born with congenital syphilis • 1985-1990: overall incidence ↑ 75% ( Sex-Drug traffic)
IncidenceUS • 1998: 81.3% of reported cases of CS occurred because the mother received no/inadequate penicillin tx before or during pregnancy • According to the CDC: • 40% of births are stillborn • 40-70% of the survivors will be infected • & 12% of these will subsequently die
Reported cases for infants < 1 year of age and rates of 1ry & 2ry syphilis among women: United States, 1997–2006
Rates for infants < 1 year of age: US, 1997–2006 and the Healthy People 2010 target as per STD surveillance
Incidence International • Worldwide, predominantly in large cities • Certain European countries have seen ↑in congenital syphilis cases • Major public health problem in sub-Saharan Africa and developing world • Main focus in control: Antenatal screening & treatment of infected mothers
PathophysiologyCS • Trans placental transmission • Transmission rate:~ 60 - 100% • With early onset disease, manifestations result from trans placental spirochetemia and are analogous to secondary stage of acquired syphilis • CS does not have a primary stage
Clinical Manifestations • Intra-uterine: -Placenta -Fetus • Post-natal: - Early - Late
Intra-uterine: Placenta • The placenta is typically large and edematous • Characteristic placental findings include: - Hydrops placentalis • Chronic villitis • Perivillous fibrous proliferation • Normoblastemia • Necrotizing funisitis • Acute chorioamnionitis • Plasma cell deciduitis
Intra-uterine: Fetus • Depends on stage of development at time of infection & duration of untreated infection • Initially characterized by placental involvement and hepatic dysfunction (e.g., abnormal LFT), followed by amniotic fluid infection, hematologic abnormalities, ascites, and hydrops • Stillbirth / Neonatal death
Intra-uterine: Fetus • >24 weeks gestation: 66 % of fetuses have either congenital syphilis or T.Pallidum detected in amniotic fluid • Intrauterine death: 25 % of affected • Perinatal mortality: 25-30 %, if untreated
Post-Natal • Among survivors, manifestations been divided into: Early stage = First 2 years Late stage = After 2 years • Inflammatory changes do not occur in the fetus until after first trimester → organogenesis is unaffected • Nevertheless, all organ systems may be involved
Early CS- Asymptomatic • Occurs between 0 - 2 years • If asymptomatic : - Identified on routine prenatal screening - If not identified and treated, these newborns develop poor feeding and rhinorrhea ➨ Earliest signs of CS may be poor feeding and snuffles (i.e., syphilitic rhinitis)
Symptomatic Early CS If Symptomatic: • Variable • Appear within 1st 5 weeks of life • Stillborn/ Premature • Failure to gain weight or FTT • Fever / Irritability • Severe congenital pneumonia
Symptomatic Early CS • Most striking lesions affect the mucocutaneous tissues and bones: - Mucous patches - Rhinitis =snuffle - Condylomatous lesions ➨ ➨ highly characteristic features of mucous membrane involvement in CS
Symptomatic Early CS • Snuffles → Followed quickly by diffuse maculopapular desquamative rash that involves extensive sloughing of the epithelium, on the palms & soles and around the mouth & anus • When chronic → “Saddle Nose” • Lesions & nasal fluid: highly infectious
Symptomatic Early CS • Bullous skin disease known as “pemphigus syphiliticus” ➲ Early rash -- small blisters on the palms and soles → Ulcerated ➲ Later rash -- copper-colored, flat or bumpy rash on the face, palms, and soles
Symptomatic Early CS • Other early manifestations include hepatosplenomegaly (100%), jaundice, anemia • Metaphyseal dystrophy and periostitis often are noted on radiographs at birth +/_ Pseudoparalysis
Congenital syphilis - early evidence of infection - bullae and vesicular rash
Multiple, punched out, pale, blistered lesions, with associated desquamation of palms & plantars
Secondary lesions on feetLesions first appeared during 4th week
Late-onset CS • Develop from scarring related to early infection • Can be prevented by treatment within first 3 months • Can appear as late as 40 years after
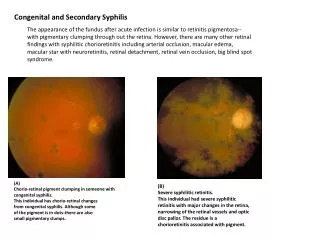
Late-onset CS • Manifestations include neurosyphilis and involvement of teeth, bones, eyes, and 8th cranial nerve • E.g.: Frontal bossing, short maxilla, high palatal arch, Hutchinson triad, saddle nose, and perioral fissure (Rhagades = bacterial infection of skin lesions )
Hutchinson triad • Deafness (10 – 40 years) • Hutchinson’s teeth = centrally notched, widely-spaced peg-shaped upper central incisors • Interstitial Keratitis → blindness (5-20 years)
Metaphyseal osteomyelitis Radiolucent distal radius & ulna with cupping distal ulna
1-m-old . Classical Wimberger's sign of destructive metaphysitis involving medial aspects of distal femora and proximal tibae
Possible Complications • Blindness • Deafness • Facial deformity • Neurological problems
Labs Definitive diagnosis: • By direct visualization of spirochetes using darkfield microscopy • Or direct fluorescent antibody tests of lesion exudate or tissue (Placenta/UC) -Helpful early in the disease, prior to development of seroreactivity
Serologic tests - Presumptive diagnosis can be made using • Nontreponemal ( False + in medical conditions) • Treponemal (False+ in other spirochetal Diseases) → So use of only one type is insufficient - If nontreponemal test is +→ confirmatory testing is performed with a specific treponemal test
Nontreponemal test • VDRL (Venereal Disease Research Laboratory) • RPR (Rapid plasma reagin) • ART (Automated reagin test)
Nontreponemal test - Used for screening (sensitive but not specific) - Inexpensive, performed rapidly, and provide quantitative results → helpful indicators of disease activity & monitor treatment response • Measures Ab directed against lipoidal Ag from T. Pallidum, Ab interaction with host tissues or both - Nonspecific Ab develop 4-8 weeks following infection
False negative Early primary S Latent acquired S Late CS Prozone phenomenon False Positive Viral infection ( EBV, Hepatitis, Varicela, Measles) Lymphoma TB Malaria Endocarditis CT diseases Pregnancy IV drugs Wharton Jelly contamination in cord samples Nontreponemal test
Nontreponemal test • Any reactive NT test must be confirmed by Treponemal test to exclude false positive • Treatment should not be delayed if symptomatic or at high risk of infection • Monitor: • Sustained 4 fold ↓NT test titer after treatment → Adequate treatment - Sustained ↑: Re-infection or relapse
Nontreponemal testNewborn Dilemma • Testing of newborn often is problematic because IgG antibody may be a reflection of maternal rather than infant infection • Unless NT titer is much higher in baby than in mother → f/u serology over 1st 6 months of life, when maternal IgG is lost, would be required to make a diagnosis i.e.Loosing precious time in treatment initiation
Treponemal Specific Test • T pallidum immobilization (TPI) • Fluorescent treponemal antibody absorption (FTA-ABS) • Microhemagglutination assay for antibodies to T pallidum (MHA-TP)
Treponemal Specific Test • Confirm + nontreponemal reaginic test • Remain positive for life i.e. Result do not correlate with disease activity and tests are not quantified • False + reactions: → Other spirochetal diseases (e.g., yaws, pinta, leptospirosis, rat-bite fever, relapsing fever, Lyme disease