Download
1 / 28
550 likes | 2.35k Views
SESSION 5 Dermatomes & myotomes Forearm & hand. Introduction. What is a spinal nerve, dermatome, myotome? Dermatomes and myotomes of the upper limb Testing function of dermatomes and myotomes Clinical importance of dermatomes Cubital fossa Carpal tunnel

E N D
SESSION 5 Dermatomes & myotomes Forearm & hand
Introduction • What is a spinal nerve, dermatome, myotome? • Dermatomes and myotomes of the upper limb • Testing function of dermatomes and myotomes • Clinical importance of dermatomes • Cubital fossa • Carpal tunnel • Some clinical notes on the forearm and hand
What is a spinal nerve? • “Mixed nerve” afferent/sensory & efferent/motor, somatic & autonomic • Runs between a specific vertebral level and the body hence “segmental nerve”
What is a dermatome? • “Skin segment” • An area of skin innervated by the cutaneous branches of a single spinal nerve • Every spinal nerve except C1 innervates a dermatome
What is a myotome? • The muscle equivalent • A muscle mass innervated by the motor branches of a single spinal nerve
Learning dermatomes • Be able to draw dermatomes on a blank diagram • Be able to show the position of a dermatome on a person • OSCE!
Learning dermatomes • Pictures in text books vary! • LMS likes ‘Clinically Oriented Anatomy’ which likes the Foerster and • Keegan & Garrett models • Learn one but be aware that other representations exist
Dermatomes of the upper limb • The limbs receive their nerves from nerve plexuses (e.g. brachial plexus) • Spinal nerve roots join & split • Terminal branches contain fibres from more than one spinal nerve “multi-segmental peripheral nerves”
Dermatomes of the upper limb • Dermatomes C5-T1 are supplied via branches of the brachial plexus • Overlap NOT at the axial line
Cutaneous peripheral nerve vs. dermatome distribution M Median nerve, C6-8 Radial nerve, C6-8 Ulnar nerve, C8 & T1 multi-segmental peripheral nerves C6 U M C8 R U C7 R Dermatome distribution of the hand
Clinical relevance?! • A nerve lesion proximal to the brachial plexus affects a spinal nerve and its individual dermatome and/or myotome • A nerve lesion distal to the brachial plexus affects a multi-segmental peripheral nerve and its distribution • Nerve lesions present with paraesthesia/anaesthesia and/or weakness/paralysis in their regions of innervation
Testing skin sensation • Pain • pin prick Temperature • test tube of hot water • something metal and cold Light touch • wisp of cotton wool • Areas where dermatome overlap is minimal: • C5; upper lateral aspect of arm • C6; pad of thumb • C7; pad of third finger • C8; pad of little finger • T1; medial aspect of elbow
Testing myotomes • Selected joint movements against resistance • Symmetrical? • Particular myotomes affected? • Proximal/distal/general weakness? • Muscle stretch reflexes • Absent/present/reduced/increased?
Muscle stretch reflexes • Sudden stretching of a muscle usually causes rapid contraction of the muscle • Tendon hammer • Biceps jerk • C5, C6 • Triceps jerk • C7, C8
Clinical importance • Nerve lesions • Sensory effects: paraesthesia, anaesthesia • Motor effects: weakness, paralysis
Clinical importance • Referred pain • Injury to visceral structures can present as vague pain in a distant area • Spinal nerves are mixed • Myocardial infarction • Myocardium is innervated by nerve fibres from spinal nerves T1-T5 • The brain perceives pain as coming from the dermatomes of T1-T5 • Pain felt in chest; referred to left arm
Summary • Dermatome is an area of skin innervated by the cutaneous branches of a single spinal nerve • Dermatomes and their spinal nerves are assessed using pain, temperature and light touch • Myotome is a muscle mass innervated by the motor branches of a single spinal nerve • Specific joint movements assess integrity of myotomes and their respective nerves
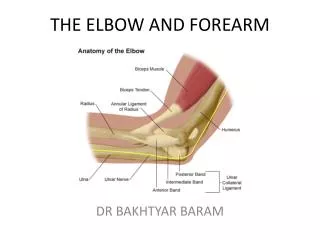
Pulled elbow What: Subluxation of the radial head The anular ligament tears Pain: If free anular ligament is compressed between capitulum and radial head Who: Children under 5 years of age How: Pulling a child’s hand in pronated position (e.g. when child is pulled up a curb) Treatment: Supination and flexion of the elbow joint (in a sling)
Scaphoid fracture History fall on outstretched hand; tender anatomical snuffbox Relatively poor blood supply, primarily from radial artery; artery enters distal pole of bone and passes proximally; fracture across the narrow waist can cause avascular necrosisaof proximal segment Fracture difficult to see on x-ray before bone resorption; “wrist sprain” misdiagnosis Without complication, healing takes 3 months
Carpal tunnel Sidewalls Concavity of carpal bones Floor Carpal bones Roof Flexor retinaculum (prevents tendons from bowing) Contents 9 flexor tendons 4 FD profundus 4 FD superficialis 1 flexor pollicis longus 1 nerve Median nerve
Carpal tunnel syndrome What: Entrapment syndrome due to pressure on the median nerve in the carpal tunnel Possible causes: Tenosynovitis, repetitive trauma, oedema, fractures, dislocation Risk factors: RA, pregnancy, obesity Clinical presentation: Sensory effect – paraesthesia/anaesthesia in lateral 3 ½ digits Motor effect – progressive weakness in thumb; inability to oppose thumb Treatment: Prevent cause of increased pressure, e.g. inflammation Carpal tunnel release N.B.: Muscles innervated by the median nerve proximal to the carpal tunnel remain unaffected (e.g. FDS) Median nerve’s palmar cutaneous branch overlies flexor retinaculum i.e. does not pass through carpal tunnel, so central palm sensation is unaffected
Colles’ fracture What: Transverse fracture of the distal 2cm radius How does it occur: Fall on outstretched hand in pronation Forced wrist dorsi-flexion Clinical presentation: Dinner fork deformity “Posterior angulation just proximal to wrist” Reason for dinner fork deformity: • Comminuted distal radial fragment Dorsal displacement • Radial shortening Ulnar styloid process often avulsed Ulna projects further distally than radius
Tenosynovitis Cause: Infection of the distal synovial sheath Presentation: Subcutaneous inflammation, the digit swells and movement is painful Infection spread: • Synovial sheath > common flexor sheath > carpal tunnel > forearm Connection between synovial sheath and common flexor sheath? • NO: tendons of digits 2, 3 & 4 • YES: tendons of digit 5 • Synovial sheath of FPL > forearm • Ruptured inflamed sheath > hand compartment