Download
1 / 14
140 likes | 295 Views
Impact of Setting and Clinical Information on ECG Interpretation. R. Roberts, M. Everett ,R. McNutt, , T. Kirages, A. Papadapolos, R. Rydman, R. Doug Scott. Introduction. Accurate ECG assessment is paramount ECGs provide key information important in: Thrombolytics

E N D
Impact of Setting and Clinical Information on ECG Interpretation R. Roberts, M. Everett ,R. McNutt,, T. Kirages, A. Papadapolos, R. Rydman, R. Doug Scott
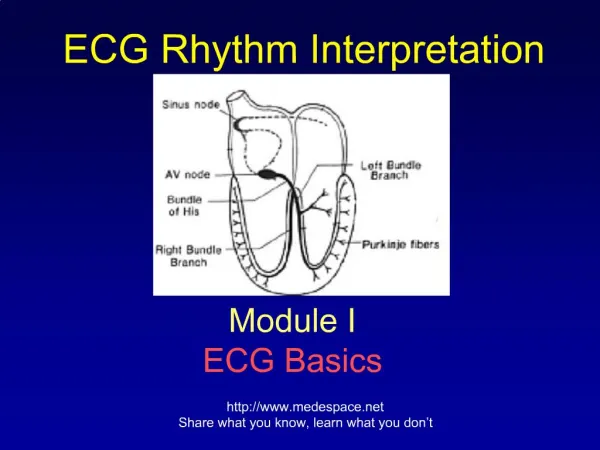
Introduction • Accurate ECG assessment is paramount • ECGs provide key information important in: • Thrombolytics • Risk Adjustment for Chest Pain • Diagnosis • Changes in clinical status
Objective • Our aim was to explore the effect of: 1) Intra-rater reliability: inter-settings (same MD, different setting) 2) Intra-rater reliability: intra-settings (same MD, same setting)
MethodsIntra-rater: inter-setting • Setting: 21 ED Physicians (MD) who documented the ECG interpretation for 1600 patients with chest pain admitted to the hospital. • We randomly selected 10 ECGs per MD originally interpreted as “abnormal” • Abnormal ECG: • Pathologic q waves • ST elevation or depression • T wave inversion (TWI) • Left Bundle Branch Block (LBBB)
MethodsIntra-rater: intra-setting Intra-rater reliability • Re-interpretation of the ECGs by the same MD in a different setting Inter-rater reliability • 10 ECGs (never seen before) were interpreted by 20 MDs on 2 separate occasions in the same setting (conference room)
Methods (1) ECG reading (real time) Randomly selected 10/ MD (2) MD rereads 2nd ECG (conference room) (3) 10 new ECGs MD reads (conference room) (4) Same 10 ECGs MD reads (conference room) Hypothesis: Difference between #1 & #2 > difference between #3 & #4 Difference is due to setting and clinical concerns
Results - Summary • Intra-rater reliability / Inter-setting: 204 ECGs Perfect Agreement 83% 12% of “Abnormal” ECGs re-read as normal • Intra-rater reliability / Intra-setting: 110 ECG Perfect Agreement 89%
ResultsSame Setting n= 209 (418 readings) p=<0.8 NS (T-test & Rank Sum) 71% ECGs 24% 4% 0% Perfect Agreement
ResultsDifferent Setting n= 239 (478 readings) p=<.001 (T-test & Rank Sum) 48% 42% ECGs 1% 7% Perfect Agreement
Conclusions • Agreement between 2 readings by the same MD is significantly greater when both readings occur in a non-clinical setting when compared to the readings between two different settings • Rates of reversal from abnormal to normal interpretations are similar to rates of reversal seen in thrombolytic trials when ECGs are re-interpreted by a central authority
Conclusions • The difference in setting and the availability of clinical information may explain some of the variability in ECG interpretation • Previous studies showing the value of ECGs in predicting patient outcome often rely upon the clinical physician’s interpretation which may be influenced by clinical information Our findings are similar to that of others
Final Thoughts • Clinical information for ECG interpretation may influence patient outcomes • Quality assurance is tied to clinical factors and settings
Limitations • We used abnormal ECGs: “stacked the deck” • All patients were admitted • Future studies: • Larger sample • Include patients sent home • Study impact on patient outcomes and resource utilization