Download
1 / 1

E N D
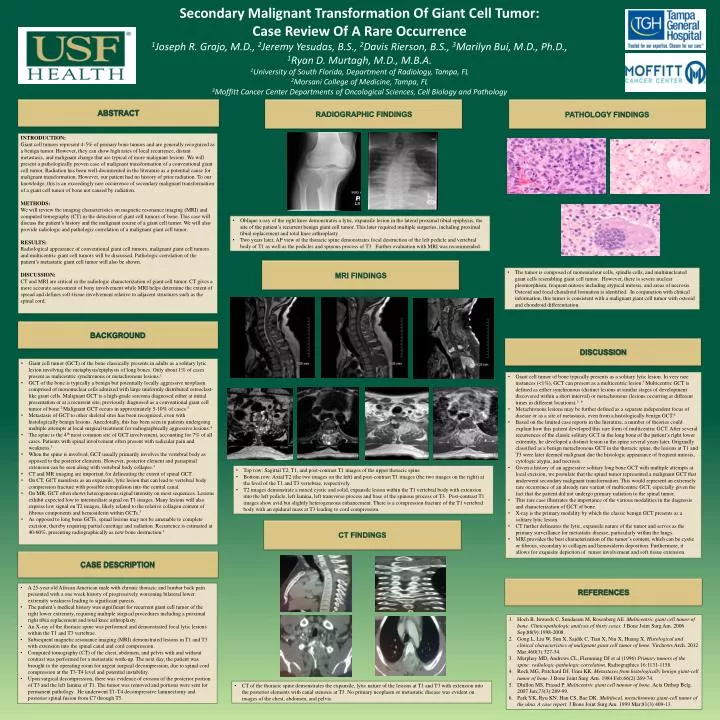
Secondary Malignant Transformation Of Giant Cell Tumor: Case Review Of A Rare Occurrence1Joseph R. Grajo, M.D., 2Jeremy Yesudas, B.S., 2Davis Rierson, B.S., 3Marilyn Bui, M.D., Ph.D., 1Ryan D. Murtagh, M.D., M.B.A.1University of South Florida, Department of Radiology, Tampa, FL2Morsani College of Medicine, Tampa, FL3Moffitt Cancer Center Departments of Oncological Sciences, Cell Biology and Pathology ABSTRACT RADIOGRAPHIC FINDINGS PATHOLOGY FINDINGS INTRODUCTION: Giant cell tumors represent 4-5% of primary bone tumors and are generally recognized as a benign tumor. However, they can show high rates of local recurrence, distant metastasis, and malignant change that are typical of more malignant lesions. We will present a pathologically proven case of malignant transformation of a conventional giant cell tumor. Radiation has been well-documented in the literature as a potential cause for malignant transformation. However, our patient had no history of prior radiation. To our knowledge, this is an exceedingly rare occurrence of secondary malignant transformation of a giant cell tumor of bone not caused by radiation. METHODS:We will review the imaging characteristics on magnetic resonance imaging (MRI) and computed tomography (CT) in the detection of giant cell tumors of bone. This case will discuss the patient’s history and the malignant course of a giant cell tumor. We will also provide radiologic and pathologic correlation of a malignant giant cell tumor. RESULTS:Radiological appearance of conventional giant cell tumors, malignant giant cell tumors and multicentric giant cell tumors will be discussed. Pathologic correlation of the patient’s metastatic giant cell tumor will also be shown. DISCUSSION: CT and MRI are critical in the radiologic characterization of giant cell tumor. CT gives a more accurate assessment of bony involvement while MRI helps determine the extent of spread and defines soft-tissue involvement relative to adjacent structures such as the spinal cord. • Oblique x-ray of the right knee demonstrates a lytic, expansile lesion in the lateral proximal tibial epiphysis, the site of the patient’s recurrent benign giant cell tumor. This later required multiple surgeries, including proximal tibial replacement and total knee arthroplasty • Two years later, AP view of the thoracic spine demonstrates focal destruction of the left pedicle and vertebral body of T1 as well as the pedicles and spinous process of T3. Further evaluation with MRI was recommended. MRI FINDINGS • The tumor is composed of mononucleur cells, spindle cells, and multinucleated giant cells resembling giant cell tumor. However, there is severe nuclear pleomorphism, frequent mitosis including atypical mitosis, and areas of necrosis. Osteoid and focal chondroid formation is identified. In conjunction with clinical information, this tumor is consistent with a malignant giant cell tumor with osteoid and chondroid differentiation. BACKGROUND DISCUSSION • Giant cell tumor (GCT) of the bone classically presents in adults as a solitary lytic lesion involving the metaphysis/epiphysis of long bones. Only about 1% of cases present as mulicentric synchronous or metachronous lesions.1 • GCT of the bone is typically a benign but potentially locally aggressive neoplasm comprised of mononuclear cells admixed with large uniformly distributed osteoclast-like giant cells. Malignant GCT is a high-grade sarcoma diagnosed either at initial presentation or at a recurrent site, previously diagnosed as a conventional giant cell tumor of bone.2 Malignant GCT occurs in approximately 5-10% of cases.3 • Metastasis of GCT to other skeletal sites has been recognized, even with histologically benign lesions. Anecdotally, this has been seen in patients undergoing multiple attempts at local surgical treatment for radiographically aggressive lesions.4 • The spine is the 4th most common site of GCT involvement, accounting for 7% of all cases. Patients with spinal involvement oftenpresent with radicular pain and weakness.3 • When the spine is involved, GCT usually primarily involves the vertebral body as opposed to the posterior elements. However, posterior element and paraspinal extension can be seen along with vertebral body collapse.3 • CT and MR imaging are important for delineating the extent of spinal GCT. • On CT, GCT manifests as an expansile, lytic lesion that can lead to vertebral body compression fracture with possible retropulsion into the central canal. • On MR, GCT often shows heterogeneous signal intensity on most sequences. Lesions exhibit expected low to intermediate signal on T1images. Many lesions will also express low signal on T2 images, likely related to the relative collagen content of fibrous components and hemosiderin within GCTs.3 • As opposed to long bone GCTs, spinal lesions may not be amenable to complete excision, thereby requiring partial curettage and radiation. Recurrence is estimated at 40-60%, presenting radiographically as new bone destruction.3 • Giant cell tumor of bone typically presents as a solitary lytic lesion. In very rare instances (<1%), GCT can present as a multicentric lesion.5 Multicentric GCT is defined as either synchronous (distinct lesions at similar stages of development discovered within a short interval) or metachronous (lesions occurring at different times in different locations).5,6 • Metachronous lesions may be further defined as a separate independent focus of disease or as a site of metastasis, even from a histologically benign GCT.6 • Based on the limited case reports in the literature, a number of theories could explain how this patient developed this rare form of multicentric GCT. After several recurrences of the classic solitary GCT in the long bone of the patient’s right lower extremity, he developed a distinct lesion in the spine several years later. Originally classified as a benign metachronous GCT in the thoracic spine, the lesions at T1 and T3 were later deemed malignant due the histologic appearance of frequent mitosis, cytologic atypia, and necrosis. • Given a history of an aggressive solitary long bone GCT with multiple attempts at local excision, we postulate that the spinal tumor represented a malignant GCT that underwent secondary malignant transformation. This would represent an extremely rare occurrence of an already rare variant of multicentric GCT, especially given the fact that the patient did not undergo primary radiation to the spinal tumor. • This rare case illustrates the importance of the various modalities in the diagnosis and characterization of GCT of bone. • X-ray is the primary modality by which the classic benign GCT presents as a solitary lytic lesion. • CT further delineates the lytic, expansile nature of the tumor and serves as the primary surveillance for metastatic disease, particularly within the lungs. • MRI provides the best characterization of the tumor’s content, which can be cystic or fibrous, secondary to collagen and hemosiderin deposition. Furthermore, it allows for exquisite depiction of tumor involvement and soft tissue extension. • Top row: Sagittal T2, T1, and post-contrast T1 images of the upper thoracic spine • Bottom row: Axial T2 (the two images on the left) and post-contrast T1 images (the two images on the right) at the level of the T1 and T3 vertebrae, respectively. • T2 images demonstrate a mixed cystic and solid, expansile lesion within the T1 vertebral body with extension into the left pedicle, left lamina, left transverse process and base of the spinous process of T3. Post-contrast T1 images show avid but slightly heterogeneous enhancement. There is a compression fracture of the T1 vertebral body with an epidural mass at T3 leading to cord compression. CT FINDINGS CASE DESCRIPTION REFERENCES • A 25-year old African American male with chronic thoracic and lumbar back pain presented with a one week history of progressively worsening bilateral lower extremity weakness leading to significant paresis. • The patient’s medical history was significant for recurrent giant cell tumor of the right lower extremity, requiring multiple surgical procedures including a proximal right tibia replacement and total knee arthroplasty. • An X-ray of the thoracic spine was performed and demonstrated focal lytic lesions within the T1 and T3 vertebrae. • Subsequent magnetic resonance imaging (MRI) demonstratedlesions in T1 and T3 with extension into the spinal canal and cord compression. • Computed tomography (CT) of the chest, abdomen, and pelvis with and without contrast was performed for a metastatic work-up. The next day, the patient was brought to the operating room for urgent surgical decompression, due to spinal cord compression at the T3-T4 level and potential instability. • Upon surgical decompression, there was evidence of erosion of the posterior portion of T3 and the left lamina of T1. The tumor was removed andportions were sent for permanent pathology. He underwent T1-T4 decompressive laminectomy and posterior spinal fusion from C7 through T5. • Hoch B, Inwards C, Sundaram M, Rosenberg AE. Multicentric giant cell tumor of bone. Clinicopathologic analysis of thirty cases. J Bone Joint Surg Am. 2006 Sep;88(9):1998-2008. • Gong L, Liu W, Sun X, Sajdik C, Tian X, Niu X, Huang X. Histological and clinical characteristics of malignant giant cell tumor of bone.Virchows Arch. 2012 Mar;460(3):327-34. • Murphey MD, Andrews CL, Flemming DJ et al (1996) Primary tumors of the spine: radiologic-pathologic correlation.Radiographics 16:1131-1158. • Rock MG, Pritchard DJ, Unni KK. Metastases from histologically benign giant-cell tumor of bone. J Bone Joint SurgAm. 1984 Feb;66(2):269-74. • Dhillon MS, Prasad P. Multicentric giant cell tumour of bone. ActaOrthop Belg. 2007 Jun;73(3):289-99. • Park YK, Ryu KN, Han CS, Bae DK. Multifocal, metachronous giant-cell tumor of the ulna. A case report.J Bone Joint Surg Am. 1999 Mar;81(3):409-13. • CT of the thoracic spine demonstrates the expansile, lytic nature of the lesions at T1 and T3 with extension into the posterior elements with canal stenosis at T3. No primary neoplasm or metastatic disease was evident on images of the chest, abdomen, and pelvis.