Download
1 / 12
120 likes | 238 Views
Prehospital Fibrinolysis with Double Antiplatelet Therapy in Acute ST-Elevation Myocardial Infarction: The Clarity Ambulance Substudy. Ambulance Substudy Background.

E N D
Prehospital Fibrinolysis with Double Antiplatelet Therapy in Acute ST-Elevation Myocardial Infarction: The Clarity Ambulance Substudy
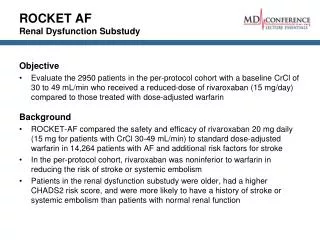
Ambulance Substudy Background • Fibrinolysis for ST-elevation acute myocardial infarction (STEMI) is frequently limited by delays of administration as well as incomplete reperfusion or reocclusion of the infarct-related artery1 • Intensified prehospital management may shorten time to treatment and improve outcomes2 1. Brouwer MA et al. Circulation 2002; 106: 659–665. 2. Morrison LJ et al. JAMA 2000; 283: 2686–2692.
Substudy Sites and Patient Numbers France: 172 patients • L Soulat: 57 • Y Lambert: 48 • F Lapostolle: 28 • F Thieuleux: 21 • C Gully: 10 • D Pollet: 5 • D Galley: 2 • L Olliver: 1 • UK: 40 patients • J Adgey: 27 • J Purvis: 13 • Sweden: 5 patients • J-E Karlsson: 5 217 patients in total
Patient Management: Ambulancevs. Non-Ambulance *p <0.001 versus ambulance patients; values are median unless otherwise specified
0 0.5 1.0 1.5 2.0 2.5 3.0 Angiographic & ECG Parameters: Ambulance vs. Non-Ambulance Event rate (%) Odds ratio (95% CI) Ambulance Non-ambulance p value Ambulance better Non-ambulance better *Complete considered to be >70%; ECG=electrocardiogram
0 0.5 1.0 1.5 2.0 2.5 3.0 Primary Outcome Parameters: Ambulance vs.Non-Ambulance Event rate (%) Odds ratio (95% CI) Ambulance Non-ambulance p value Non-ambulance better Ambulance better *Occluded infarct artery (TFG 0/1) + death + re-MI prior to angiography; NS=not significant
0 0.5 1.0 1.5 2.0 2.5 3.0 Primary Outcome Parameters: Ambulance Subgroup Event rate (%) Odds ratio (95% CI) Clopidogrel Placebo p value Placebo better Clopidogrel better *Occluded infarct artery (TFG 0/1) + death + re-MI prior to angiography
Primary Endpoint of TIMI Flow Grade 0/1, MI or Death Odds ratio (95% CI) 0.60 (0.301.17) Ambulance 0.65 (0.540.77) Non-ambulance Overall 0.64 (0.530.76) 0 0.5 1.0 1.5 2.0 Clopidogrel better Placebo better
Safety: Bleeding Complications TIMI=thrombolysis in myocardial infarction; ICH=intracranial hemorrhage
Conclusions • Medical reperfusion of STEMI patients with fibrinolysis, heparin, ASA and clopidogrel is feasible before reaching the hospital in medically equipped ambulances without an apparent increase in bleeding • Early management of patients in the ambulance is associated with shorter ischaemic times and faster reperfusion, with a consistent treatment effect in favour of clopidogrel in comparison with the overall results