Download
1 / 28
280 likes | 507 Views
http://www.dcss.cs.amedd.army.mil/field/FLIP%20Disk%2041/FLIP.html. http://www.dcss.cs.amedd.army.mil/field/FLIP%20Disk%2041/FLIP.html. Idiopathic Membranous Nephropathy. Paul M. Johnson UNC Internal Medicine AM Report August 4, 2009. Overview. Epidemiology Pathophysiology

E N D
http://www.dcss.cs.amedd.army.mil/field/FLIP%20Disk%2041/FLIP.htmlhttp://www.dcss.cs.amedd.army.mil/field/FLIP%20Disk%2041/FLIP.html
http://www.dcss.cs.amedd.army.mil/field/FLIP%20Disk%2041/FLIP.htmlhttp://www.dcss.cs.amedd.army.mil/field/FLIP%20Disk%2041/FLIP.html
IdiopathicMembranous Nephropathy Paul M. Johnson UNC Internal Medicine AM Report August 4, 2009
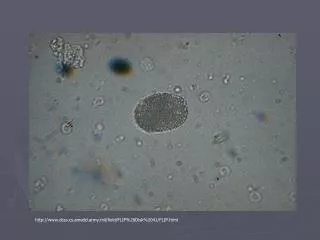
Overview • Epidemiology • Pathophysiology • Clinical Presentation • Diagnosis/Work Up • Prognosis • Treatment • Our patient…6 months later Oval fat body under polarized light showing maltese cross.
Epidemiology • 13.4 cases per million in adults • onset most commonly 4th to 5th decade (idiopathic) • 75% idiopathic • FSGS has overtaken MN as most common cause of nephrotic syndrome in adults • 2:1 males : females
Secondary Membranous Nephropathy Ponticelli C. Membranous nephropathy J Nephrol 2007;20:268-287.
Pathophysiology • circulating IgG antibodies directed against endogenous antigens on or near podocyte foot processes form immune complexes • C5b-9 (MAC) causes cell signaling -> • silt diaphragm protein disruption • redistribution of actin • GBM expansion by injured podocytes • antigens?: dsDNA, thyroglobulin, hepatitis B surface antigen, treponemal antigen, and not yet discovered….
Pathophysiology • Glassock RJ. N Engl J Med 2009;361:81-83.
Membranous Nephropathy thick GBM (in relation to tubular basement membrane) mesangial expansion (asterisks) Normal Glomerulus thin GBM (equivalent to tubular basement membrane) mesangium limited to stalk of capillary tuft (double arrows) images from www.uptodate.com
Immunofluorescence diffuse granular IgG deposits along GBM Silver Stain spike pattern in GBM highlights deposits between new GBM images from www.uptodate.com
Membranous EM thick GMB, with deposits (D) effacement of foot processes Normal EM thin, homogenous GBM epithelial cell with foot processes fenestrated endothelial cell (arrow)
Clinical Presentation • 80% present with nephrotic syndrome • hypoalbuninemia and hyperlipidemia most often present • sublinical to more than 20 g/day of proteinuria • 70% have normal BP and normal GFR
Diagnosis/Work Up • U/A, microscopy, UP/C • > 3.5 g/day • oval fat bodies, lipid droplets, fatty casts • Rule Out Secondary Causes • ANA/Complement • SPEP/UPEP • Hepatitis Serologies, RPR, HIV • cyroglobulins
Diagnosis/Work Up • Kidney biopsy is needed for diagnosis, and should be done in all patients with unexplained nephrotic syndrome • Lipids • 5-20% over 65 have malignancy • age appropriate screening
Prognosis • “rule of thirds” • complete: 5-30% at 5 y • partial: (<2 g) 25-40% at 5 y • ESRD: 14% at 5 y, 35% 10 y, 41 % 15 y • Toronto Glomerulonephritis Registry Schieppati, A, et al, N Engl J Med 1993; 329:85. Figure www.uptodate.com
Good Prognosis female young age normal creatinine <4 g proteinuria /day for 6 mos no tubulointerstitial disease Poor Prognosis > 8 g proteinuria/day for 6 months Prognosis Creatinine levels in patient with complete remission of idiopathic membranous nephropathy Ponticelli C. J Nephrol 2007;20:268-287.
Treatment: Low Risk • ACE I or ARB: act, at least in part, to lower intraglomerular pressure • Goal BP <130/80 • may require diuretics • Lipid-lowering: statins most often needed • low salt diet • anticoagulation: controversial • highest risk: >12 g/day, albumin <2
Treatment: Moderate and High Risk • Moderate: 4-8 g/day x 6 months • (45% will have spontaneous remission) • if no better in 6 mos: immunosuppression • High: > 8 g/day x 6 months or worsening renal function • (75% progress to ESRD) • cyclophosphamide OR cyclosporine/tacrolimus PLUS glucocorticoids • trial of rituximab • Transplant: if ESRD – 10-30% recurrence
Our Patient….. • UP/C is 5.12 (almost 50% reduction) • Creatinine stable • CH 238, HLD 95, LDL 125 • Taking enalapril 10, lipitor 40 • Continues to ride long distances on bike
Key Points • Membranous nephropathy only about ¼ of all causes of nephrotic syndrome • 75% idiopathic, but must rule out secondary causes • Rule of Thirds • Treat symptoms of low risk patients • Immunosuppression in high risk patieints
References • www.uptodate.com • Schieppati, A, Mosconi, L, Perna, A, et al, N Engl J Med 1993; 329:85. • Ponticelli C. Membranous nephropathy J Nephrol 2007;20:268-287. • Wasserstein AG. Membranous glomerulonephritis J Am Soc Nephrol 1997;8:664-674. • Glassock RJ. Human idiopathic membranous nephropathy--a mystery solved? N Engl J Med 2009;361:81-83.