Download
1 / 27
510 likes | 2.64k Views
MECHANISM OF LABOUR (NORMAL & ABNORMAL). Presented By Dr. ZEINAB ABOTALIB MRCOG, DGO, Associate Professor & Consultant Obs/Gyna Infertility & IVF. Lie, presentation, attitude, &position . FETAL LIE The relation of the long axis of the fetus to that of the mother

E N D
MECHANISM OF LABOUR (NORMAL & ABNORMAL) Presented By Dr. ZEINAB ABOTALIB MRCOG, DGO, Associate Professor & Consultant Obs/Gyna Infertility & IVF
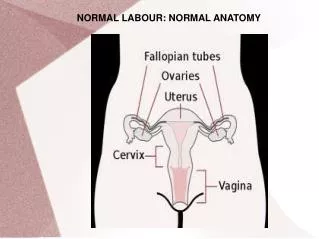
Lie, presentation, attitude, &position FETAL LIE • The relation of the long axis of the fetus to that of the mother • Longitudinal lie is found in 99% of labours at term • Predisposing factors for transverse lie/oblique lie multiparity, placenta previa, hydramnious, & uterine anomalies FETAL PRESENTATION • The presenting part is the portion of the body of the fetus that is foremost in the birth canal • The presenting part can be felt through the Cx on vaginal examination • Longitudinal lie cephalic presentation breech presentation • Transvrse lie shoulder presentation
Lie, presentation, attitude, &position CEPHALIC PRESENTATION • Head is flexed sharply vertex / occiput presentation • Head is extended sharply face presentation • Partially flexed bregma presenting (sinciput presentation) • Partially extended brow presentation BREECH PRESENTATION • Frank breech • Complete breech • Footling breech ATTITUDE • Posture of the fetus folded on itself to accommodate the shape of the uterus • Flexed head, thighs, knees &feet • The arms crossed over the chest • Face presentation extended concave contour of the vertebral column
(A) vertex (B) sinciput (C) brow (D) face
POSITION The relation of an arbitrary chosen point of the fetal presenting part to the Rt or Lt side of the maternal birth canal The chosen point • Vertex presentation occiput • Face presentation mentum • Breech presentation Sacrum Each presentation has two positions Rt or Lt Each position has 3 varieties : Ant, transverse, post OA ROA LOA ROT LOT ROP LOP OP
A. Right occiput posterior (ROP) Right occiput transverse (ROT)
FREQUENCY OF VARIOUS PRESENTATIONS & POSITIONS AT TERM • Vertex 96% 2/3 Lt 1/3 Rt • Breech 3.5% • Face 0.3% • Shoulder0.4%
Lt mento-ant Rt mento-ant Rt mento-post
MECHANISM OF LABOUR WITH OCCIPUT PRESENTATIONSTHE CARDINAL MOVEMENTS OF LABOUR 1-ENGAGEMENT The greatest transverse diameter BPD passes through the pelvic inlet It may occur in the last few weeks of pregnancy or only in labour especially in multipara The fetus enters the pelvis in transverse or oblique diameter • LOT 40% • ROT 20% • OP 20% ROP >LOP • ROA / LOA20%
THE CARDINAL MOVEMENTS OF LABOUR • Asynclitism The sagittal sutures of the head deflects ant towards the symphysis pubis or post towards the sacrum 2-DESCENT • In nullipara engagement takes place before the onset of labour & further descent may not occur till the 2nd stage • In multipara descent begins with engagement • It is gradually progressive till the fetus is delivered • It is affected by the uterine contractions & thinning of the lower segment
3-FLEXION • The descending head meets resistance of pelvic floor, Cx & walls of the pelvis flexion • The shorter suboccipito-begmatic is substituted for the longer occipito-frontal
4-INTERNAL ROTATION • Turning of the head from the OT position anteriorly towards the symphysis pubis ie. Occiput moves from transverse to ant 45º • Less commonly OT posteriorly towards the sacrum 135º • It is not accomplished till the head has reached the spines The levator ani muscles form a V shaped sling that tend to rotate the vertex anteriorly • It is completed by the time the head reaches the pelvic floor 2/3 or shortly after ¼
EXTENSION • When the flexed head reaches the vulva it undergoes extension the base of the occiput will be in direct contact with the inferior margin of the symphysis pubis • Crowning the largest diameter of the fetal head is encircled by the vulvar ring • The head is born by further extension as the occiput, bregma, forehead, nose, mouth & chin pass successively over the perineum
EXTERNAL ROTATIONRESTITUTION • After delivery of the head it returns to the position it occupied at engagement , the natural position relative to the shoulders (oblique position)Restitution • Then the fetal body will rotate to bring one shoulder anterior behind the symphysis pubis ( biacromial diameter into the APD of the pelvic outlet) • Restitution is followed by complete external rotation to transverse position (occiput lies to next to Lt maternal thigh) • The ant shoulder slips under the pubis • By lateral flexion of the fetal body the post shoulder will be delivered & the rest of the body will follow
OCCIPUT POSTERIOR POSITION • Mechanism of labour is identical to OT & anterior varieties • The occiput rotate to the symphysis pubis through 135º instead of 90º or 45º • If rotation does not occur direct occiput post or Partial rotation transverse arrest