Download
1 / 28
280 likes | 566 Views
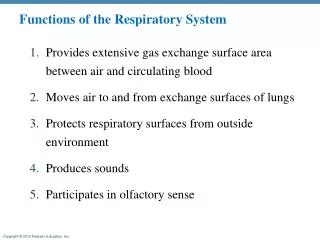
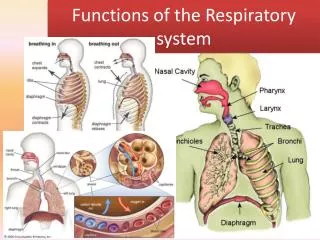
Respiratory System Primary functions Move oxygen from air to cells Move carbon dioxide from cells to air Secondary Functions Warm, cleanse and humidify air Regulate plasma levels of H+ ion Control of body temperature (not much in humans) Speech.

E N D
Respiratory System Primary functions Move oxygen from air to cells Move carbon dioxide from cells to air Secondary Functions Warm, cleanse and humidify air Regulate plasma levels of H+ ion Control of body temperature (not much in humans) Speech
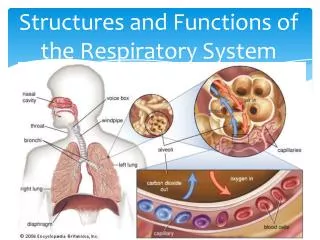
Respiratory and Conducting Zones Cartilage in trachea and large bronchi Airway resistance – bronchioles (autonomic effects) Mucociliary system
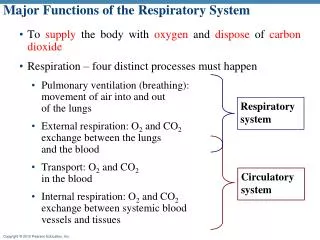
Respiratory Mechanics Air is a gas mixture Gases and liquids are fluids Fluids always move “downhill” in a pressure gradient Therefore, any time a fluid moves, the pressure is higher in the place it leaves than in the place it goes Pressures relevant to respiration Atmospheric (average, 760 mm Hg) Pulmonary (= alveolar) Intrapleural When pulmonary > atmospheric, air leaves lungs When pulmonary < atmospheric, air enters lungs
Elasticity of the lungs Natural tendency is to collapse. Prevented by negative pressure in (air tight) thoracic cavity. Boyle’s Law: Pressure exerted by a gas mixture on the walls of a container is directly proportional to number of molecules of the gas and inversely proportional to the volume of the container. As thorax expands, intrapleural pressure falls (fewer gas molecules per unit volume). As thorax contracts, intrapleural pressure rises.
Elasticity of the lungs (continued) Why are lungs elastic? 1. Elastic fibers in outer wall 2. La Place’s Law: In a sphere containing a fluid, surface tension creates a force tending to collapse the sphere (increases the pressure inside it) 3. Pressure resulting from surface tension increases as volume of the sphere decreases 4. Alveoli are tiny spheres. Therefore, surface tension at the gas-liquid interface in them creates high pressure, driving air out and tending to collapse the lungs 5. Collapse is prevented by thorax being air tight. When punctured, thoracic pressure reaches atmospheric and lungs collapse
Which direction will air flow if the stopcock is opened? Why?
Which direction will air flow if the stopcock is opened? Why? Have you never blown up a balloon? (poor thing!)
Pulmonary Surfactant: Alveoli in newborns are fully collapsed, so their volume is small and the surface tension opposing their expansion is high Pulmonary surfactant reduces the surface tension (detergents are surfactants; they reduce surface tension between grease on your dishes and the water used to clean them) Pulmonary surfactant production begins around the end of the 7th month of gestation Hence, birth is delayed until 7 months gestation whenever possible
Muscles in Breathing At rest – diaphragm contracts during inspiration, relaxes for expiration Mild activity – external intercostal muscles contract during inspiration, relax during expiration Slightly strenuous activity – internal intercostal muscles contract during expiration Strenuous activity – muscles of upper chest and neck contract during inspiration, relax during expiration. Abdominal muscles contract during expiration In normal breathing, inspiration is active, expiration is passive
What affects rate of air movement? Pressure difference between alveoli and atmosphere (normally varies between +2 cm H2O and -2 cm H2O) Airway resistance – mainly in bronchioles, where it can vary (sympathetic stimuli relax bronchiolar smooth muscle, parasympathetic stimuli contract it) Obstructive pulmonary disorders are those where airway resistance is high (asthma, for example). Muscular effort is required to expire; wheezing Normal people use 3%-5% of their daily caloric expenditure for breathing. In obstructive disorders it can reach 30%, even at rest
Control of Airway Resistance Autonomic input to bronchiolar smooth muscle Smooth muscle responses to local oxygen and CO2 levels
FEV1 = Volume that can be forcibly exhaled from maximally inflated lungs in one second. FEV1 is about 80% of vital capacity in healthy people FEV1 can be as low as 50% of vital capacity in people with obstructive disorders FEV1 is about 80% of vital capacity in people with restrictive disorders, but vital capacity is reduced
Anatomical Dead Space Conducting zone volume = 150 ml The final 150 ml of each inspiration never gets into the respiratory zone The last 150 ml expired never leaves the lungs, and re-enters the respiratory zone on the next inspiration Therefore, if tidal volume = 500 ml, only 350 ml of fresh air enters respiratory zone. The conducting zone is, therefore, called the anatomical dead space
Unless tidal volume exceeds dead space, no fresh air reaches the alveoli More dead space can result from breathing through a tube (Can you hide in a swamp by submerging and breathing through a hollow reed? How does a deep sea diver manage to survive with the huge dead space of the air hose connected to his helmet?)
Alveolar Ventilation vs. Pulmonary Ventilation Pulmonary ventilation rate = respiration rate x tidal volume. Typically around 6 liters/min (12 breaths x 500 ml tidal volume) Alveolar ventilation rate = respiration rate x (tidal volume – dead space) Typically around 4200 ml/min (12 breaths x (500 ml tidal volume – 150 ml dead space)) Note different effects of increasing tidal volume vs increasing respiration rate. Under most circumstances, we automatically optimize both for efficiency
Concentrations of Gases in Liquids How to deal with diffusion between a gas and a liquid? Need for common units of concentration Basic gas law: pressure exerted by every molecule in a gas mixture is the same. Therefore, if one gas is 20% of the total in a mixture, it exerts 20% of the total pressure. The pressure exerted by each gas in a mixture is called its partial pressure. Oxygen is about 20% of the molecules in air. Total pressure in air at sea level is about 760 mm Hg. Therefore, partial pressure of oxygen = PO2 = 152 mm Hg
What determines oxygen concentration in water equilibrated with oxygen-containing gas mixture? Since the force driving O2 into the water is its partial pressure, the concentration will be proportional to PO2 The other factor is the relative solubilities of oxygen in air (in which it is high) and in water (in which it is low) When the system is in equilibrium, the force driving oxygen into the water (PO2) must be equal to the force driving oxygen out of the water. Therefore, we can refer to the concentration of oxygen in water in terms of PO2.
Since oxygen diffuses into the alveolar capillaries, PO2 in alveolar air must be greater than PO2 in alveolar capillaries. PO2 in alveolar air is about 100 mm Hg. Why isn’t it about 150 mm Hg, as in room air? Because only 70% of the air in the alveoli is fresh air (dead space, remember?) What’s the PO2 in blood entering alveolar capillaries? We’ll come back to that, but it’s much less than 100 mm Hg. What’s the PO2 in blood leaving the alveolar capillaries? It’s about 100 mm Hg; the air and the blood in the alveoli equilibrate. This is made possible by the very high ratio of surface to volume in alveoli.
Oxygen Transport in Blood With PO2 = 100 mm Hg, amount of oxygen dissolved in water (or plasma) = 0.3% by volume. That’s 3 ml per liter of plasma. Since cardiac output is about 5 liters/min, oxygen can be delivered at a maximum rate of 15 ml/minute if it’s dissolved in plasma. Normal resting oxygen consumption is about 300 ml/min. Wait a minute! That’s 20x as fast as it can be delivered. It’s possible, though, because most oxygen in the blood isn’t dissolved in plasma, it’s reversibly bound to hemoglobin. Hemoglobin is a protein in red blood cells. It gives them their red color.
Hemoglobin’s reversible binding of oxygen can be represented as a reversible equation, Hb + O2 HbO2 In pulmonary capillaries, where PO2 is 100 mm Hg, this equilibrium is pushed to the right. Hemoglobin “loads” oxygen. In fact, it becomes nearly saturated with it. In systemic capillaries, where PO2 is much lower, hemoglobin “unloads” oxygen, which can then diffuse out of the red cells, across the capillaries and into the interstitial fluid, and into the cells.
Fetal hemoglobin has higher affinity for oxygen than adult hemoglobin does – that’s why fetus can get oxygen delivered to its tissues Bohr effect: Oxygen-hemoglobin saturation curve shifts to right (hemoglobin affinity for oxygen decreases) as local CO2 level goes up. Since PCO2 goes up in the systemic capillaries and down in the alveolar capillaries, hemoglobin “loads” more readily in the latter, “unloads” more readily in the former. Neatly adaptive. Bohr thought this was an effect of CO2 on hemoglobin. But CO2 + H2O H2CO3 (Carbonic acid) H+ + HCO3- (bicarbonate) Bohr effect is actually due to increased H+ when CO2 increases
CO2 + H2O H2CO3 H+ + HCO3- Happens spontaneously, but is accelerated by the enzyme, carbonic anhydrase in biological systems.
CO2 Transport in Blood Forms of CO2 in blood: About 10% is dissolved CO2 About 30% is bound to hemoglobin (so-called carbamino compounds) About 60% is bicarbonate ion In alveoli: PO2 is high in alveolar air, low in alveolar plasma. Therefore, O2 diffuses into capillaries PCO2 is high in alveolar plasma, low in alveolar air. Therefore, CO2 diffuses out of plasma. Because PCO2 is reduced in alveolar plasma, blood leaving the alveolar capillaries has lower H+ concentration than blood entering it.
Control of Respiration Neural: Inspiratory center in brainstem causes diaphragm to contract about every 5 seconds (12 times per minute) You can easily modify depth and rate of respiration voluntarily, but can’t suspend respiration for more than a minute or so. Why not? Obvious candidates are that low PO2 triggers respiration or that high PCO2 does it. We have O2 and CO2 receptors. Which is the trigger? “Shallow water blackout” demonstrates that you will lose consciousness from low PO2 before the oxygen sensors trigger respiration.