Download
1 / 34
350 likes | 672 Views
THE SHOULDER COMPLEX. SHOULDER COMPLEX. Anatomy of shoulder complex allows for a great degree of mobility. Because of the great degree of mobility, stability is sacrificed. Overuse injuries are common. BONES OF SHOULDER COMPLEX. CLAVICLE SCAPULA HUMERUS. SHOULDER COMPLEX ARTICULATIONS.

E N D
SHOULDER COMPLEX • Anatomy of shoulder complex allows for a great degree of mobility. • Because of the great degree of mobility, stability is sacrificed. • Overuse injuries are common
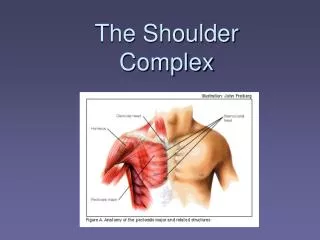
BONES OF SHOULDER COMPLEX • CLAVICLE • SCAPULA • HUMERUS
SHOULDER COMPLEX ARTICULATIONS • Sternoclavicular • Acromioclavicula • Glenohumeral • Scapulothoracic
Glenohumeral Joint Movements Flexion Extension Abduction Adduction External Rotation Internal Rotation Circumduction
Movements Cont. • Horizontal Abduction • Horizontal Adduction • Elevation • Depression • Protraction • Retraction
Glenohumeral Joint Muscles • Originates in axial skeleton and inserts on the humerus • Latissmus dorsi- internal rotation, extension. • Pectoralis major- horizontal adduction, flexion.
Glenohumeral Joint Muscles • Originates on Scapula and attach to Humerus • Anterior Deltoid • Abduction • Flexion • Lateral Deltoid • Abduction • Posterior Deltoid • Abduction • Extension
Glenohumeral Joint Muscles • Teres Major • Internal Rotation • Extension • Coracobrachialis • Flexion • Horizontal Adduction
Glenohumeral Joint Muscles • Rotator Cuff • Supraspinatus • Abduction • External Rotation • Infraspinatus • External Rotation • Extension • Teres minor • External Rotation • Extension • Subscapularis • Flexion • Internal Rotation
Glenohumeral Joint Muscles • Originates on Axial Skeleton Insertion point on Scapula • Levator Scapula • Elevation • Trapezius • Part 1: Elevation • Part 2: Elevation, Adduction of Scapula • Part 3: Adduction of Scapula • Part 4: Depression, Adduction of Scapula
Glenohumeral Joint Muscles • Rhomboids • Adduction of Scapula • Elevation • Serratus anterior • Abduction of Scapula
Acromioclavicular Ligaments • Coracoacromial ligament • Acromioclavicular ligament • Coracoclavicular ligament
Prevention of Shoulder Injuries • Proper physical conditioning • Strengthen shoulder muscles through the full Range of Motion. • Proper warm-up and Stretch • Falling properly (ie shoulder roll) • Properly fitted protective equipment • Proper technique
Correct Throwing Technique • Wind-up Phase • Cocking Phase • Acceleration • Deceleration • Follow Through
Wind-up Phase • First movement until ball leaves gloved hand • Lead leg strides forward • Both shoulders abduct, externally rotate, and horizontally abduct.
Cocking Phase • Hands separate until maximal external rotation of the humerus • Foot comes in contact with ground
Acceleration • Maximum external rotation until ball is released • Humerus abducts, horizontally abducts and internally rotates. • Scapula elevates, abducts, and upward rotates.
Deceleration • Ball release until maximal shoulder internal rotation. • External rotators act as decelerators by eccentrically contracting
Follow Through • Last phase of throwing • Maximum internal rotation until the end of the motion. • Balanced position • Important phase to avoid throwing injuries.
Assessing the Shoulder • One of the most difficult regions of the body to evaluate.
HISTORY • What happened to cause this pain? • Have you ever had this problem? • What is the duration and intensity of pain? • Where is pain located? • Is there crepitus during movement or numbness or distortion in temperature such as a cold or warm feeling?
HISTORY • Is there a feeling of weakness or a sense of fatigue? • What shoulder movements or positions seem to aggravate or relieve the pain? • If therapy has been given before, what, if anything offered pain relief?
ANTERIOR OBSERVATION • Are both shoulder tips even with one another? • Is one shoulder held higher because of muscle spasm or guarding? • Is the lateral end of the clavicle prominent? • Is one lateral acromion process more prominent that the other?
ANTERIOR OBSERVATION • Does the clavicular shaft appear deformed? • Is there loss of the normal lateral deltoid muscle contour? • Is there an indentation in the upper biceps region?
LATERAL OBSERVATON • Is there thoracic kyphosis or are the shoulders slumped forward? • Is there forward or backward arm hang?
POSTERIOR OBSERVATION • Is there asymmetry such as a low shoulder, uneven scapulae, or winging of one scapular wing and not the other? • Is the scapula protracted because of constricted pectoral muscles? • Is there a distracted or winged scapula on one or both sides?
PALPATION • Done anteriorly and posteriorly • Both shoulder are palpated at same time for pain sites and deformities. • Detects point tenderness, abnormal swelling or lumps, muscle spasm or guarding, and trigger points.
SPECIAL TESTS • Active and passive range of motion should be noted and compared to opposite side. • Strength of the of the shoulder musculature should be assessed by resisted manual muscle testing.
APPREHENSION TEST (crank test) • With arm abducted 90 degrees. • Shoulder is slowly and gently externally rotated as far as the athlete will allow. • Athlete with anterior glenohumeral instability will show apprehension before end point can be reached.
Test for Shoulder Impingement • Forced flexion of the humerus in the overhead position may cause impingement of soft tissue structures. • Horizontal adduction with forced internal rotation of the humerus.
Test for Supraspinatus Muscle Weakness • Empty Can Test: • Bring both arms in to 90 degrees of forward flexion • 30 degrees of horizontal abduction • Arms are internally rotated as far as possible, thumbs pointing down. • Downward pressure applied. • Arms should be the same strength.