Download
1 / 37
370 likes | 682 Views
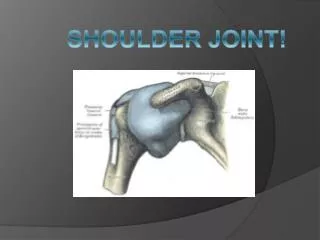
Chapter 18: The Shoulder Complex. Shoulder Joint-Anatomy (1). Sternum Clavicle Scapula- acromion process and coracoid process, glenoid fossa and glenoid labrium, spine of scapula Humerus- Greater tubercle, Lesser tubercle, head of humerus,

E N D
Shoulder Joint-Anatomy (1) • Sternum • Clavicle • Scapula- acromion process and coracoid process, glenoid fossa and glenoid labrium, spine of scapula • Humerus- Greater tubercle, Lesser tubercle, head of humerus, • http://www.readingshoulderunit.com/shoulder_anatomy.htm
Sternoclavicular (SC) Joint ** • ___________________________________ • Allows for rotation during movements like shrugging the shoulders and reaching above the head. • Supported by 4 ligaments- • __________________________________ • Costoclavicular ligament • Interclavicular ligament
Acromioclavicular (AC) Joint** • Lies between the acromion process and the clavicle • ______________________ • Primary ligament: ________________ • Secondary ligaments • Coracoacromial ligament • Coracoclavicular ligaments
Glenohumeral (GH) Joint**(1) • ___________________________ • Glenoid fossa of the scapula • ____________________ • Head of the humerus (3-4 x larger than glenoid)-plunger/volleyball example • _________________________
GH joint** (2) • Joint is deepened by a meniscus like structure called the glenoid labrum • functions to add stability to the joint • Stabilized by two types of stabilizers • Static stabilizers • joint capsule • several glenohumeral ligaments
GH joint** (3) • Dynamic stabilizers • rotator cuff muscles (SITS) • _______________ • _______________ • _______________ • _______________
Other shoulder anatomy (3) • Bursa • _______________ (clinically most important) • Nerve supply • brachial plexus (________) • Blood supply • _____________________________
Shoulder movements • Flexion (180) and Extension (80-90) • Abduction (180) and Adduction • Horizontal Adduction/Flexion (130) • Horizontal Abduction/Extension (60) • External rotation (90) • Internal rotation (90)
ROM/Muscle Testing • Shoulder flexion- __________________ • Shoulder extension-Post Delt • Shoulder abduction-____________________ • Shoulder adduction- ___________________ • Shoulder internal rotation-Ant Delt/ Subscapularis • Shoulder external rotation- ____________________________________ • Horizontal ADD/Flex- ________________ • Horizontal ABD/Ext- _________________ • Scapula elevation, depression, protraction, and retraction
Apprehension test (Crank test) • Apprehension test used for anterior glenohumeral instability • This motion should not be forced
Test for Shoulder Impingement • Neer’s test and Hawkins-Kennedy test for impingement used to assess impingement of soft tissue structures • Positive test is indicated by pain and grimace
Test for Supraspinatus Weakness • Empty Can Test • 90 degrees of shoulder flexion, internal rotation and 30 degrees of horizontal adduction • Downward pressure is applied • Weakness and pain are assessed bilaterally
Special Test Continue • Yerguson’s • Drop Arm
Prevention of Shoulder Injuries • Proper physical conditioning is key • Develop body and specific regions relative to sport • Warm-up should be used before explosive arm movements are attempted • _____________________________________________________________________ • Protective equipment • ________________________________
Preventing shoulder problems • General muscle strengthening • Try and avoid exercises above 90 degrees in the beginning • Stretching for shoulder capsule, but be careful • Strengthening rotator cuff muscles • including eccentric work • http://www.asmi.org/SportsMed/throwing/thrower10.html • Throwing Program • Strengthen scapular stabilizers • push-ups • press-ups
Throwing Mechanics • Instruction in proper throwing mechanics is critical for injury prevention
Windup Phase • First movement until ball leaves gloved hand • Lead leg strides forward while both shoulders abduct, externally rotate and horizontally abduct • Cocking Phase • Hands separate (achieve max. external rotation) while lead foot comes in contact w/ ground • Acceleration • Max external rotation until ball release (humerus adducts, horizontally adducts and internally rotates) • Scapula elevates and abducts and rotates upward
Deceleration Phase • Ball release until max shoulder internal rotation • Eccentric contraction of ext. rotators to decelerate humerus while rhomboids decelerate scapula • Follow-Through Phase • End of motion when athlete is in a balanced position
Recognition and Management of Specific Injuries • Clavicular Fractures • Cause of Injury • ____________________________, fall on tip of shoulder or direct impact • Occur primarily in middle third (greenstick fracture often occurs in young athletes) • Signs of Injury • _____________________________________________________________________________ • Clavicle may appear lower • Palpation reveals pain, swelling, deformity and point tenderness
Clavicular Fractures (continued) • Care • Closed reduction - sling and swathe, immobilize w/ figure 8 brace for 6-8 weeks • Removal of brace should be followed w/ joint mobes, isometrics and use of a sling for 3-4 weeks • Occasionally requires operative management
Sternoclavicular Sprain • Cause of Injury • Indirect force, blunt trauma (may cause displacement) • Signs of Injury • Grade 1 - pain and slight disability • Grade 2 - pain, subluxation w/ deformity, swelling and point tenderness and decreased ROM • Grade 3 - gross deformity (dislocation), pain, swelling, decreased ROM • Possibly life-threatening if dislocates posteriorly • Care • PRICE, immobilization • Immobilize for 3-5 weeks followed by graded reconditioning
Acromioclavicular Sprain • Cause of Injury • Result of direct blow (from any direction), upward force from humerus, FOOSH • Signs of Injury • Grade 1 - point tenderness and pain w/ movement; no disruption of AC joint • Grade 2 - tear or rupture of AC ligament, partial displacement of lateral end of clavicle; pain, point tenderness and decreased ROM (abduction/adduction) • Grade 3 - Rupture of AC and CC ligaments with dislocation of clavicle; gross deformity (Step deformity);+ Piano Key Test, pain, loss of function and instability
Care • Ice, stabilization, referral to physician • Grades 1-3 (non-operative) will require 3-4 days (grade 1) and 2 weeks of immobilization ( grade 3) • Aggressive rehab is required w/ all grades • ______________________________________________________________________________ • Progress as athlete is able to tolerate w/out pain and swelling • _________________________________________________________________________
Glenohumeral Dislocations • Cause of Injury • Head of humerus is forced out of the joint • Anterior dislocation is the result of an anterior force on the shoulder, forced abduction, extension and external rotation • Occasionally the dislocation will occur inferiorly (Hill-Sachs Lesion vs Bankart Lesion vs SLAP Tears) • Signs of Injury • Flattened deltoid, prominent humeral head in axilla; arm carried in slight abduction and external rotation; moderate/severe pain and disability • Care • RICE, immobilization and reduction by a physician • Begin muscle re-conditioning ASAP • Use of sling should continue for at least 1 week • Progress to resistance exercises as pain allows
Shoulder Impingement Syndrome • Cause of Injury • Mechanical compression of supraspinatus tendon, Glenoid labrum, subacromial bursa and long head of biceps tendon due to decreased space under coracoacromial ligament • _________________________________________________________________________ • Signs of Injury • Diffuse pain, pain on palpation of subacromial space; • Decreased strength of external rotators compared to internal rotators; tightness in posterior and inferior capsule • _______________________________________
Care • Restore normal biomechanics in order to maintain space • Strengthening of rotator cuff and scapula stabilizing muscles • Stretching of posterior and inferior joint capsule • Modify activity (control frequency and intensity)
Rotator cuff tear • Involves supraspinatus or rupture of other rotator cuff tendons • Primary mechanism - acute trauma (high velocity rotation- degrees per sec??????) • Occurs near insertion on greater tuberosity • Full thickness tears usually occur in those athletes w/ a long history of impingement or instability • Signs of Injury • Present with pain with muscle contraction • Tenderness on palpation and loss of strength due to pain • Loss of function, swelling • With complete tear impingement and empty can test are positive
Care • RICE for modulation of pain • Progressive strengthening of rotator cuff • Reduce frequency and level of activity initially with a gradual and progressive increase in intensity
Shoulder Bursitis • Etiology • ___________________________________________________________________________ • May develop from direct impact or fall on tip of shoulder • Signs of Injury • ___________________________________________________________________________ • Management • Cold packs and NSAID’s to reduce inflammation • Remove mechanisms precipitating condition • Maintain full ROM to reduce chances of contractures and adhesions from forming
Bicipital Tendonitis • Cause of Injury • Repetitive overhead athlete - ballistic activity that involves repeated stretching of biceps tendon causing irritation to the tendon and sheath • Signs of Injury • ______________________________________________________________________ • ___________________________________ • ____________________________ • Care • Rest and ice to treat inflammation • NSAID’s • Gradual program of strengthening and stretching