Download
1 / 1
10 likes | 100 Views
Trends and determinants of severe morbidity in HIV-infected patients: emerging role of bacterial infections, cardiovascular and psychiatric diseases: ANRS CO3 Aquitaine Cohort, 2000-2004.

E N D
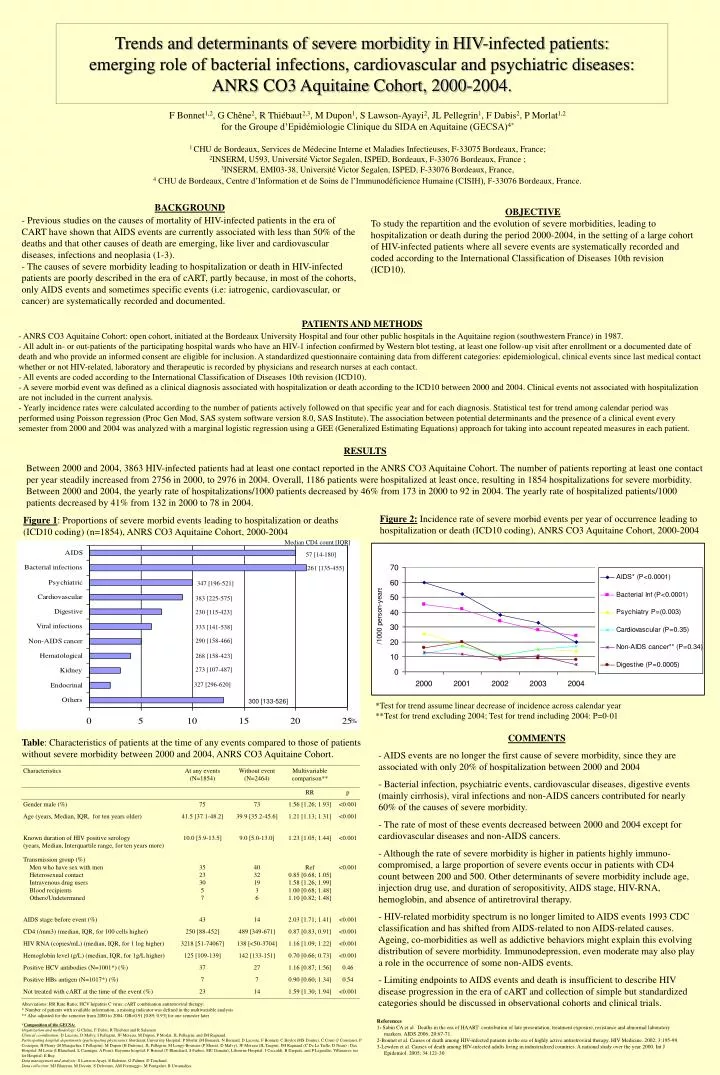
Trends and determinants of severe morbidity in HIV-infected patients: emerging role of bacterial infections, cardiovascular and psychiatric diseases: ANRS CO3 Aquitaine Cohort, 2000-2004. F Bonnet1,2, G Chêne2, R Thiébaut2,3, M Dupon1, S Lawson-Ayayi2, JL Pellegrin1, F Dabis2, P Morlat1,2 for the Groupe d’Epidémiologie Clinique du SIDA en Aquitaine (GECSA)4* 1 CHU de Bordeaux, Services de Médecine Interne et Maladies Infectieuses, F-33075 Bordeaux, France; 2INSERM, U593, Université Victor Segalen, ISPED, Bordeaux, F-33076 Bordeaux, France ; 3INSERM, EMI03-38, Université Victor Segalen, ISPED, F-33076 Bordeaux, France, 4 CHU de Bordeaux, Centre d’Information et de Soins de l’Immunodéficience Humaine (CISIH), F-33076 Bordeaux, France. • BACKGROUND • Previous studies on the causes of mortality of HIV-infected patients in the era of CART have shown that AIDS events are currently associated with less than 50% of the deaths and that other causes of death are emerging, like liver and cardiovascular diseases, infections and neoplasia (1-3). • The causes of severe morbidity leading to hospitalization or death in HIV-infected patients are poorly described in the era of cART, partly because, in most of the cohorts, only AIDS events and sometimes specific events (i.e: iatrogenic, cardiovascular, or cancer) are systematically recorded and documented. OBJECTIVE To study the repartition and the evolution of severe morbidities, leading to hospitalization or death during the period 2000-2004, in the setting of a large cohort of HIV-infected patients where all severe events are systematically recorded and coded according to the International Classification of Diseases 10th revision (ICD10). • PATIENTS AND METHODS • - ANRS CO3 Aquitaine Cohort: open cohort, initiated at the Bordeaux University Hospital and four other public hospitals in the Aquitaine region (southwestern France) in 1987. • All adult in- or out-patients of the participating hospital wards who have an HIV-1 infection confirmed by Western blot testing, at least one follow-up visit after enrollment or a documented date of death and who provide an informed consent are eligible for inclusion. A standardized questionnaire containing data from different categories: epidemiological, clinical events since last medical contact whether or not HIV-related, laboratory and therapeutic is recorded by physicians and research nurses at each contact. • All events are coded according to the International Classification of Diseases 10th revision (ICD10). • A severe morbid event was defined as a clinical diagnosis associated with hospitalization or death according to the ICD10 between 2000 and 2004. Clinical events not associated with hospitalization are not included in the current analysis. • - Yearly incidence rates were calculated according to the number of patients actively followed on that specific year and for each diagnosis. Statistical test for trend among calendar period was performed using Poisson regression (Proc Gen Mod, SAS system software version 8.0, SAS Institute). The association between potential determinants and the presence of a clinical event every semester from 2000 and 2004 was analyzed with a marginal logistic regression using a GEE (Generalized Estimating Equations) approach for taking into account repeated measures in each patient. RESULTS Between 2000 and 2004, 3863 HIV-infected patients had at least one contact reported in the ANRS CO3 Aquitaine Cohort. The number of patients reporting at least one contact per year steadily increased from 2756 in 2000, to 2976 in 2004. Overall, 1186 patients were hospitalized at least once, resulting in 1854 hospitalizations for severe morbidity. Between 2000 and 2004, the yearly rate of hospitalizations/1000 patients decreased by 46% from 173 in 2000 to 92 in 2004. The yearly rate of hospitalized patients/1000 patients decreased by 41% from 132 in 2000 to 78 in 2004. Figure 2: Incidence rate of severe morbid events per year of occurrence leading to hospitalization or death (ICD10 coding), ANRS CO3 Aquitaine Cohort, 2000-2004 Figure 1: Proportions of severe morbid events leading to hospitalization or deaths (ICD10 coding) (n=1854), ANRS CO3 Aquitaine Cohort, 2000-2004 Median CD4 count [IQR] 57 [14-180] 261 [135-455] 347 [196-521] 383 [225-575] 230 [115-423] 333 [141-538] 290 [158-466] 268 [158-423] 273 [107-487] 327 [296-620] 300 [133-526] *Test for trend assume linear decrease of incidence across calendar year **Test for trend excluding 2004; Test for trend including 2004: P=0·01 % • COMMENTS • AIDS events are no longer the first cause of severe morbidity, since they are associated with only 20% of hospitalization between 2000 and 2004 • Bacterial infection, psychiatric events, cardiovascular diseases, digestive events (mainly cirrhosis), viral infections and non-AIDS cancers contributed for nearly 60% of the causes of severe morbidity. • The rate of most of these events decreased between 2000 and 2004 except for cardiovascular diseases and non-AIDS cancers. • Although the rate of severe morbidity is higher in patients highly immuno-compromised, a large proportion of severe events occur in patients with CD4 count between 200 and 500. Other determinants of severe morbidity include age, injection drug use, and duration of seropositivity, AIDS stage, HIV-RNA, hemoglobin, and absence of antiretroviral therapy. • HIV-related morbidity spectrum is no longer limited to AIDS events 1993 CDC classification and has shifted from AIDS-related to non AIDS-related causes. Ageing, co-morbidities as well as addictive behaviors might explain this evolving distribution of severe morbidity. Immunodepression, even moderate may also play a role in the occurrence of some non-AIDS events. • Limiting endpoints to AIDS events and death is insufficient to describe HIV disease progression in the era of cART and collection of simple but standardized categories should be discussed in observational cohorts and clinical trials. Table: Characteristics of patients at the time of any events compared to those of patients without severe morbidity between 2000 and 2004, ANRS CO3 Aquitaine Cohort. Abreviations: RR Rate Ratio; HCV hepatitis C virus; cART combination antiretroviral therapy; * Number of patients with available information, a missing indicator was defined in the multivariable analysis ** Also adjusted for the semester from 2000 to 2004: OR=0.91 [0.89; 0.93] for one semester later References 1- Sabin CA et al. Deaths in the era of HAART: contribution of late presentation, treatment exposure, resistance and abnormal laboratory markers. AIDS 2006; 20:67-71. 2-Bonnet et al. Causes of death among HIV-infected patients in the era of highly active antiretroviral therapy. HIV Medicine. 2002; 3:195-99. 3-Lewden et al. Causes of death among HIV-infected adults living in industrialized countries. A national study over the year 2000. Int J Epidemiol. 2005; 34:121-30. *Composition of the GECSA: Organization and methodology: G Chêne, F Dabis, R Thiebaut and R Salamon Clinical coordination: D Lacoste, D Malvy, I Pellegrin, JF Moreau, M Dupon, P Morlat, JL Pellegrin, and JM Ragnaud. Participating hospital departments (participating physicians): Bordeaux University Hospital: P Morlat (M Bonarek, N Bernard, D Lacoste, F Bonnet), C Beylot (MS Doutre), C Conri (J Constans), P Couzigou, H Fleury (B Masquelier, I Pellegrin), M Dupon (H Dutronc), JL Pellegrin, M Longy-Boursier (P Mercié, D Malvy), JF Moreau (JL Taupin), JM Ragnaud (C De La Taille, D Neau) ; Dax Hospital: M Loste (I Blanchard, L Caunègre, A Pons); Bayonne hospital: F Bonnal (Y Blanchard, S Farbos, MC Gemain); Libourne Hospital: J Ceccaldi, B Darpeix, and P Legendre; Villeneuve sur lot Hospital: E Buy. Data management and analysis: S Lawson-Ayayi, E Balestre, G Palmer, D Touchard. Data collection: MJ Blaizeau, M Decoin, S Delveaux, AM Formaggio, M Pontgahet, B Uwamaliya.






















