Download
1 / 33
330 likes | 414 Views
SENIORS Trial: effects of beta-blockers in elderly patients with impaired and preserved ejection fraction. Dirk J. van Veldhuisen Groningen, The Netherlands ESC-HF Nice, France June 2009 Menarini Satellite Symposium. Event free Survival %. Hazard Ratio 0.86 [0.73;0.99] p = 0.039.

E N D
SENIORS Trial:effects of beta-blockers in elderly patients with impaired and preserved ejection fraction. Dirk J. van Veldhuisen Groningen, The Netherlands ESC-HF Nice, France June 2009 Menarini Satellite Symposium
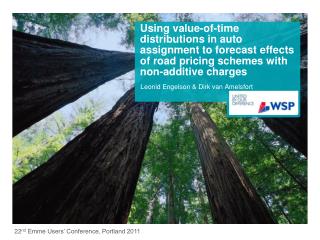
Event free Survival % Hazard Ratio 0.86 [0.73;0.99] p = 0.039 No. of events: Nebivolol 332 (31.1%); Placebo 375 (35.3%) All Cause Mortality or CV Hospital Admission (Primary Outcome)
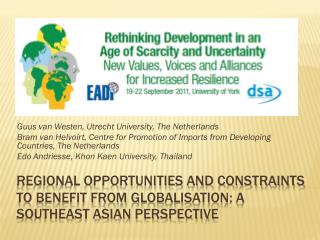
Favours Nebivolol Favours Placebo Nebivolol Placebo LVEF Age 184 (34.8%) 219 (32.1%) 332 (31.1%) 231 (35.2%) 110 (28.9%) 101 (24.6%) 148 (27.5%) 249 (36.3%) 250 (36.4%) 375 (35.3%) 125 (33.3%) 125 (33.6%) 176 (33.5%) 199 (37.1%) Male > 75 y 75 y Total 35 % > 35 % Female Sex 0.60 0.50 0.70 0.80 0.90 1.00 1.10 1.20 Death or CV Hospitalisation by Subgroup Hazard ratio and 95% CI
ESC-HF Guidelines 2008 Dickstein et al Eur J Heart Fail 2008
Terminology-Definitions • HF and Diastolic dysfunction • HF with preserved ejection fraction (HFPEF) • HF with Normal ejection fraction (HFNEF) etc. • Presence signs and symptoms • Evidence of diastolic dysfunction • Normal or only mildly abnormal LV function (LVEF ≥ 50% or 45% (or even 35-40%?)
Changes in the Population in the Netherlands (1900-2050) 1900 1950 2000 2050 (?) Source: CBS/NRC Handelsblad
Survival in HF Patients with Impaired and Preserved EF HR 0.96 Data from Owen et al. (OLMSTED County) NEJM 2006; 355: 251-9 (collected 1987-2001 Reduced EF (<50%; n=2429), preserved EF (>50%, n=2167)
Trends in Survival Rate in HF with low/high EF Data from Owen et al. (OLMSTED County) NEJM 2006; 355: 251-9 (collected 1987-2001) Reduced EF (<50%; n=2429), preserved EF (>50%, n=2167)
From: Kindermann, Böhm, Van Veldhuisen Trends Cardiovasc Med 2008
Data from Owen et al. (OLMSTED County) NEJM 2006; 355: 251-9 (collected 1987-2001 Reduced EF (<50%), preserved EF (>50%)
Signs/symptoms in HF with low & high EF Data from Bhatia et al. NEJM 2006; 355: 260-9 (collected 1999-2001)
Baseline characteristics Alternative Added PreservedOverall n=2028 n=2548 n=3023 n=7599 Mean age (years) 67 64 67 66 Women (%) 32 21 40 32 NYHA class (%) II 48 24 60 45 III 49 73 38 52 IV 3 3 2 3Mean LVEF 30 28 54 39 Medical history (%) myocardial infarction 61 56 44 53 diabetes 27 30 28 28 hypertension 50 48 64 55 atrial fibrillation 25 26 29 27
Baseline characteristics Alternative Added PreservedOverall n=2028 n=2548 n=3023 n=7599 Baseline therapy (%) ACE inhibitor 0 100 19 41 beta-blocker 55 56 56 55 diuretic 86 90 75 83 spironolactone 24 17 12 17 digitalis 46 58 28 43 aspirin 58 52 58 56 lipid lowering 41 41 42 42
CHARM-Preserved: Primary outcome CV death or CHF hospitalisation % 30 366 (24.3%) Placebo 25 333 (22.0%) 20 Candesartan 15 10 HR 0.89 (95% CI 0.77-1.03), p=0.118Adjusted HR 0.86, p=0.051 5 0 0 1 2 3 3.5 years Number at risk Candesartan 1514 1458 1377 833 182 Placebo 1509 1441 1359 824 195
Perindopril in elderly patients with HF and Preserved EF: PEP-CHF From: Cleland et al. EHJ 2006; 27: 2328-45 (LVEF >40%, 850 pts; mean age 76 years)
Irbesartan in Patients with HFPEF: I-PRESERVE 4128 pts Age 72 yr; EF 60%; 59% BB, 40% CCB Massie et al. NEJM 2008;359:2456-67
Efficay of beta-blockade in Elderly pts with HFPEF (observational data) Dobre et al Eur J Heart Fail 2006
HF with impaired (LVSD) and Preserved EF (PLVF); Observational treatment data from EuroHeart Failure Survey Lenzen et al. EHJ 2004
EF 35% EF>35% P N (% of total) 1359 (64%) 752 (36%) LVEF (mean, %) Women II NYHA Class (n, %) I III IV 405 (30%) 717 (52.8) 35 (2.6) 29 578 (42.5) 29 (2.1) 470 (62.5) 26 (3.5) 375 (50%) p<0.001 14 (1.9) p<0.001* 49 p<0.001 243 (32.2) Mean age (years) 76.1 76.1 SENIORS Baseline Characteristics by EF * Interaction test
All cause mortality or CV hospitalisation by EF EF 35% n=1359 (64%) EF > 35% n= 752 (36%) events % HR =0.86 (95% CI 0.72-1.04) HR= 0.81 (95% CI 0.63-1.04) 40 30 20 Mean EF =29% Mean EF =49% 0 0 6 12 18 24 36 0 6 12 18 24 36 0 0 Months after randomisation van Veldhuisen, Cohen-Solal, MD, Böhm et al JACC 2009 in press
SENIORS: secondary outcomes placebo
Dose-related effects of beta-blockade in patients with CHF 10 mg 5 mg 0 mg 1.25-2.5 mg Data from SENIORS. Dobre, Van Veldhuisen, Am Heart J 2007
Comorbidities in CHFRenal dysfunctionAnemiaDiabetesAtrial fibrillation
Clinical factors related to survival in low and high EF Data from Owen et al. (OLMSTED County) NEJM 2006; 355: 251-9 (collected 1987-2001 Reduced EF (<50%; n=2429), preserved EF (>50%, n=2167)
CHARM - Prognostic Value of Renal Function (GFR) Impaired LVEF Preserved LVEF Hillege et al Circulation 2006
Damaged heart after MI: LV systolic dysfunction Damaged heart after long-term hypertension: LV diastolic dysfunction
ConclusionsPatients with HFPEF have a poor prognosis; similar to those with low EF So far, conventional drugs (ACEi, ARB; proven effective for patients with low EF) are not (equally) useful for HFPEFData from SENIORS with the beta-blockernebivolol look promising in HFPEF