Download
1 / 18
180 likes | 507 Views
CT of the Right Lower Quadrant. Rajul Pandit, M.D. Acute Abdominal Pain (AAP). In 34% of cases, the cause of abdominal pain is not established Acute appendicitis is seen in 28% of AAP Acute GI and GU conditions are the most common causes of AAP

E N D
CT of the Right Lower Quadrant Rajul Pandit, M.D.
Acute Abdominal Pain (AAP) • In 34% of cases, the cause of abdominal pain is not established • Acute appendicitis is seen in 28% of AAP • Acute GI and GU conditions are the most common causes of AAP • In approximately 66% of patients with AAP diagnosis may be made on imaging findings • CT of the RLQ has effectively replaced exploratory laparotomy as the primary means of evaluating patients with a “surgical abdomen”
Acute Appendicitis (AA) • Atypical presentations result in diagnostic confusion and delay in treatment • High morbidity if perforation occurs • The diagnosis should be considered in any patient with RLQ pain unless prior appendectomy • Unusual presentations at extremes of age, pregnant patient, when appendix is distant from anterior parietal peritoneum • Diagnostic accuracy varies by sex • Negative appendectomy rates of 9% in men, 19% in women
Pathophysiology of AA • Obstruction of appendiceal lumen from fecolith, lymphoid hyperplasia, foreign bodies, parasites or tumors • Continued secretion of mucus results in elevated intraluminal pressure, venous engorgement, arterial compromise, tissue ischemia • Luminal bacteria invade the wall with transmural inflammation, perforation • Mild cases resolve if obstruction is relieved (8%) • Recurrent and chronic appendicitis seen in 1-10%
CT Technique • Thin-section (</= 5 mm), helical CT of abdomen and pelvis • Controversy over use of oral/IV contrast • IV contrast may help in mild cases of AA, minimal fat and perforating appendicitis • Oral contrast may limit false positive cases • Rectal contrast
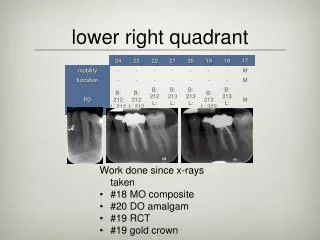
CT Criteria for AA • Distended, fluid-filled, thick-walled, tubular structure > 6mm in diameter (nl wall thickness <1-2mm) • Calcified appendicolith • Mural enhancement • Entire appendix should be seen • Periappendiceal inflammation (absent in 2-22% of cases) • Severe cases- phlegmon, abscess, extraluminal gas, ileocecal thickening, peritonitis, small bowel obstruction
Clinical Value of CT • Negative appendectomy rates have reduced to as low as 4-6 % • Cost-effective, prevents unnecessary surgery • CT differentiates abscess from phlegmon • Road-map for percutaneous abscess drainage
Right-sided Colonic Diverticulitis • Uncommon, misdiagnosed as AA • Incidence highest in Asian populations • Abnormal thickening of colon wall, pericolonic inflammation, inflamed diverticulum with marked enhancement, abscess formation • DDx difficult if normal appendix not seen
Perforated Cecal Carcinoma • 10% colorectal cancers arise in the cecum • May cause secondary appendicitis, SBO, intussusception, perforation with abscess • Large soft-tissue mass that outweighs the inflammatory component • Contiguous organ invasion, regional lymph nodes, peritoneal implants, distant mets
Cecal Infarction • Acute colonic ischemia in elderly due to low-flow states, small vessel dx • Splenic flexure most common, rare in the cecum • Cecal wall thickening, pneumatosis
Neutropenic Colitis • AKA typhlitis or ileo-cecal syndrome • Cecum mostly involved • Seen in immuno-suppressed pts. • Thickened wall, low-attenuation in the bowel wall due to edema/necrosis, pneumatosis coli, pericolonic fluid • DDx: pseudomembranous colitis, colitides by opportunistic infections like CMV
Mesenteric Adenitis and Terminal Ileitis • Mesenteric adenitis: self-limiting inflammation of the lymph nodes in children, young adults • Usually due to Campylobacter, Yersinia • Cluster of moderately enlarged lymph nodes +/- ileocecal wall thickening • DDx: Crohn’s dx
Epiploic Appendagitis • Spontaneous torsion of an epiploic appendage of the large bowel • Sudden onset of acute abdominal pain, self-limiting • Seen in 1% of patients undergoing CT for AA • Small , pedunculated, round, fat-containing mass with a hyperattenuating rim at the serosal surface of the colon • Small linear or round focus in the center of the lesion may be vascular thrombosis
Omental Infarction • Localized acute right abd pain, spontaneously resolving • Inflamed omental fat located between the right anterolateral abdominal wall and ascending colon, at or above the level of the umbilicus • High density streaks in the fat • Adjacent colon, TI and appendix are normal
Other Differentials • Sigmoid diverticulitis: LLQ pain, also in ddx for RLQ pain where the apex of the sigmoid colon may reside • Acute urinary disorders:ureteral calculi, acute pyelonephritis • Gyn conditions: ovarian cysts, torsion, PID, ectopic pregnancy