Download
1 / 68
700 likes | 814 Views
Hormones and the heart, (and other vascular things)!. Dr Heather Currie Associate Specialist Obstetrician & Gynaecologist MD Menopause Matters Ltd. Plan. CVD in women Menopause & CVD risk Menopause, HRT and other vascular things!. Demographics. 1850 Age of menopause - 45 yrs.

E N D
Hormones and the heart, (and other vascular things)! Dr Heather Currie Associate Specialist Obstetrician & Gynaecologist MD Menopause Matters Ltd
Plan • CVD in women • Menopause & CVD risk • Menopause, HRT and other vascular things!
Demographics • 1850 • Age of menopause - 45 yrs. • Life expectancy - 45 yrs. • 2009 • Age of menopause - 52 yrs. • Life expectancy - 82 yrs. • Today > 30% life = postmenopausal
Oocytes • 5th month gestation—7 million • Birth—1-2 million • Puberty—400,000 • 40+--rapid decline!
Types of menopause • Spontaneous • Surgical • Drug induced
Premature ovarian failure • Special considerations • Symptom control • Bone health • Cardiovascular health • Dementia • Fertility
Early Symptoms • Periods changing • Vasomotor • Insomnia • Mood • Connective tissue • Cognitive function • Coping
Intermediate symptoms • Urogenital atrophy • Vagina and bladder • Hugely under-reported and under-treated
Reporting and Treatment Cumming G, Currie H et al. Menopause International 2007;13:79-83
Long term health • Osteoporosis • Cardiovascular disease • Dementia
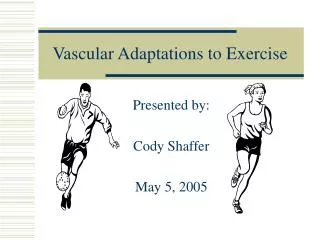
Mortality Rates in Women 6500 4500 2500 1600 1200 800 400 0 45–49 50–54 55–59 60–64 65–69 70–74 75–79 80–84 85+ At Every Age, More Women Die of Heart Disease Than Breast Cancer Coronary Artery Disease Stroke Lung Cancer Breast Cancer Colon Cancer Endometrial Cancer Mortality Rate per 100,000 Age (years) National Center for Health Statistics. 1999:164-7.
Death from CVD • Europe, stats from 2005 • 43% of men • 57% of women
Women’s perceptions of their greatest health problems Cardiovascular disease 7% Don’t know/ no answer Breast cancer 16% 34% Other problems 16% 27% Cancer Mosca et al. Arch Fam Med 2000.
European survey • Only 1/3 women associated CVD with menopause • Only ¼ associated raised cholesterol with menopause • Only 8% women 45—65 had been advised to have cholesterol level checked • Only 15% hcps aware that women equal risk as men
Symptoms of CVD in women Different from those in men Angina can be mistaken for indigestion or heartburn MI symptoms can include overwhelming fatigue, shortness of breath, nausea, or indigestion
Other problems • Often present late • Other medical problems • Poorly represented in trials • Less interventions • Worse prognosis following MI: • 38% women die in 1 year, 25% men • In 6 years, further MI in 35% women, 18% men
Incidence of CVD: Relation to Menopause Status The Framingham Study Incidence (per 1000 women) Age (years) n = 2873. Kannel WB, et al. Ann Intern Med. 1976;85:447-52.
Modifiable risk factors • Smoking • BMI (waist – hip ratio) • Lack of exercise • Hypertension • Cholesterol • Stress • Diabetes—doubles risk CVD in men, trebles risk in women
Effect of estrogen lack • Change in BMI, fat distribution • Inc LDL cholesterol • Decreased HDL • Increase TGs • Blood pressure • Glucose/insulin metabolism • 4 fold increased risk CVD • Prem menopause—53% inc risk CHD
So……… • Need for increased awareness • See onset of menopausal symptoms as “wake up call” • Think beyond symptoms • Long term health—heart as well as bones • WHO—80% CVD can be prevented by diet and lifestyle changes • Premature menopause
Contributory factors Obese population aged 15 and above • Weight • Dietary • Exercise • Smoking OECD Factbook 2005 www.sourceoecd.org/factbook
What about HRT? • Should be good! • Favourable effects on W/H ratio, lipids, vascular function, atheroma formation • Conflicting findings—observational studies and randomised trials
HRT and Cardiovascular Protection • 23 good observational studies BUT • Not randomised • Mainly unopposed estrogen • Healthy cohort effect
Effect of Duration of HT Use on Risk of Nonfatal Acute MI 0.1 0.5 1.0 2.0 5.0 Odds Ratio HT Use n = 371 Never Used n = 69 12 Months n = 75 13–60 Months n = 27 >60 Months Chilvers CE, et al. Eur Heart J. 2003;24:2197-205.
HERS: CHD Events by Year HERS HERS II Grady D, et al. JAMA. 2002;288:49-57.
HERS: Lessons Learned Hulley S, et al. JAMA. 1998;280:605-13; Grady D, et al. JAMA. 2002;288:49-57; Blumenthal RS, et al. Am J Cardiol. 2000;85:1015-7. • The women in HERS were on average 18 years postmenopause, suggesting that years since menopause may have an important influence on the cardiovascular effects associated with initiation of CEE/MPA • Cardiovascular risks of CEE/MPA in this population were observed early and did not occur in individuals taking concomitant statin therapy
Women’s Health Initiative (WHI) Clinical Trials of HT CEE = conjugated equine estrogen; MPA = medroxyprogesterone acetate; HT = hormone therapy (estrogen alone [E-alone], estrogen plus a progestin [E+P]). The Women's Health Initiative Study Group. Control Clin Trials. 1998;19:61-109. • Large, parallel, NIH-sponsored, randomized, placebo-controlled, clinical trials • CEE alone • CEE plus MPA • Purpose: Assess long-term risks and benefits of CEE alone and CEE/MPA in chronic disease prevention • More than 27,000 women aged 50 to 79 years (mean age, ~63 years) randomized between 1993 and 1998; originally scheduled to conclude in 2005 10/15/2014 10:47:24 AM
Relative Risk of CHD: Nurses’ Health Study (NHS) Versus WHI Never Users CEE Alone CEE + MPA Placebo 95% nCI CEE + MPA 95% aCI Placebo 95% nCI CEE 95% aCI NHS1 WHI E + P2 WHI E Alone3 Risk Estimate 1Manson JE, et al. N Engl J Med. 2003;349:523-34; 2Grodstein F, et al. Ann Intern Med. 2000;133:933-41; 3Women's Health Initiative Steering Committee. JAMA. 2004;291:1701-12.
WHI STUDYJAMA 2002;288:321-333 Note demographics of study population 60% > 60yrs 30% had BMI >30 Pre-existing heart disease Drop out rate 75% (active and placebo) NOV 2009 October 14
AMERICAN ENDOCRINE SOCIETY STATEMENT ON MHT JUNE 2010 • WHI data not applicable to typical women considering MHT • Av age 63 yrs. Only 3.5% 50 – 54 yrs • No assessment of symptom relief • Thus review data and new studies of MHT in women 50 - 55 yrs October 14
Does the timing of HRT matter? • Meta-analysis of 23 trials • 39,049 participants • Odds ratio for CHD differed with age at enrolment • Under 60 - 0.68—32% reduction (significant) • Over 60 - 1.03 Salpeter et al J Gen Int Med 2004;19:791-804
Timing of HRT for mortality • Meta-analysis of 30 trials • 27,000 participants • Odds ratio for mortality differed with age at enrolment • Under 60 - 0.61—significant 39% reduction • Over 60 - 1.03 • [Nurse’s Health Study HRT within 2 years of LMP - 0.63]
Effect of ERT on Coronary Atherosclerosis : Timing of Initiation Premenopausal Years Postmenopausal Years Plaque Area (% of placebo) Ovariectomy 70%1,2 1. Healthy diet CEE + atherogenic diet 2. 50%3 Atherogenic diet CEE + atherogenic diet Atherogenic diet Healthy diet+ CEE 3. 0%4 Healthy diet ~ 6 Year Human Equivalent Time 1Clarkson TB, et al. J Clin Endocrinol Metab. 1998;83:721-6; 2Adams MR, et al. Arterioscler Thromb Vasc Biol. 1997;17:217-21; 3Clarkson TB, et al. J Clin Endocrinol Metab. 2001;86:41-47; 4Williams JK, et al. Arterioscler Thromb Vas Biol. 1995;15:827-36.
Effect of Hormone Therapy on Atherosclerosis Varies With Stage of Reproductive Life Premenopause Perimenopause Postmenopause ~5% ~15% 25-35 yrs 35-45 yrs 45-55 yrs 55-65 yrs 65 yrs 15-25 yrs Benefits of Endogenous E2 Primary Benefits of HT No Benefits of HT Mikkola TS, et al. Ann Med. 2004;36:402-13.
The Effect of Body Mass on the Risk of CHD: Putting the WHI Results in Perspective BMI (kg/m2) RH = relative hazard. *Mean BMI 28.5 kg/m2. BMI data from Willett WC, et al. JAMA. 1995;273:461-5. WHI data from Manson JE, et al. N Engl J Med. 2003;349:523-34.
low-dose aspirin reduces CVA risk no reduction in CHD risk with low-dose aspirin no reduction in CHD mortality with statins reduction in CHD risk with HRT CHD: PRIMARY PREVENTION CHD Hodis and Mack. Menopause 2007; 14: 1-14
BENEFITS AND RISKS: WOMEN CHD breast cancer Hodis and Mack. Menopause 2007; 14: 1-14
Summary—HRT and CHD • Window of opportunity • Best if started within 6 years of menopause and/or before age 60 • Increased benefit with longer use • Use for at least 5 years • Results of further studies on timing, types and routes awaited • Similar risks to other commonly used drugs
Stroke • Most common cause: infarction • atheroma at branch points of cerebral arteries (carotid and vertebral) • Less common cause: ruptured aneurysm • primary intracerebral and subarachnoidal hemorrhage • Are risk factors for cerebral and myocardial infarction similar? • hypertension more important, lipids less so? • Risk factors for hemorrhagic stroke • hypertension
Ischaemic Stroke--WHI • Overall combined HRT- + 0.85/1,000/year • ---Only appreciable in 70-79 age group-extra 1.3 per 1,000 per year • Overall estrogen only- + 1.19/1,000/year • ---Only appreciable in 60-69 age group-extra 1.9 per 1,000 per year • And in 70-79 age group-extra 1.4 per 1,000 per year
Hypertension and Risk of StrokeDanish Nurse Study Lokkegaard et al Arch Neurol 2003;60:1379
Estrogen and Stroke: a case for low-dose estrogen Low doses may confer protection while higher doses may increase risk Risks may be lower with transdermal Thrombogenic effects C-reactive Protein Birge ss Menopause 2006;13(5):719-20
TRANSDERMAL AND ORAL HRT AND THE RISK OF STROKE Renoux et al, BMJ 2010; 340:83 UK GP Research Database 870,286 women with no prior stroke history aged 50 – 79 between 1987 and 2006 followed up for mean duration of 6.7 years 15710 cases of stroke October 14
TRANSDERMAL AND ORAL HRT AND THE RISK OF STROKE Low dose transdermal ET (50 micrograms) is not associated with increase in risk of stroke High dose transdermal ET and oral estrogen, alone or combined with progestogen, are associated with increased risk. Use of oral (ET or EPT) had a 28% increase in risk which translates into an absolute risk of 0.8 strokes per 1000 person years of use. October 14

![CARDIO-VASCULAR SYSTEM [CVS] FUNCTIONAL ANATOMY OF HEART](https://cdn1.slideserve.com/1739818/cardio-vascular-system-cvs-functional-anatomy-of-heart-dt.jpg)