Download
1 / 12
130 likes | 151 Views
Victorian Mental Health Service System. Sue Brennan Acting Director Mental Health 9 July 2007. Mental health – broad brush. Growing community awareness and expectations re mental health,mental illness and services

E N D
Victorian Mental Health Service System Sue Brennan Acting Director Mental Health 9 July 2007
Mental health – broad brush • Growing community awareness and expectations re mental health,mental illness and services • 19% of Victorians (1 in 5) experience some form of mental illness over lifetime (~ 3% severe;~4% moderate) • 23% of those on C/y based orders & Combined C’y & Treat’t order with MH problems; 26%+ of prison population • Mental illness is often combined with other factors which adds to complexity eg AOD, housing issues; child protection, ABI, offending/justice
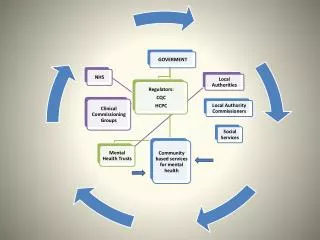
Service system broad brush • Commonwealth & State contribute (COAG) • Promotion/prevention focus & activities – Vichealth; public health; local government; other universal services eg schools • Primary mental health – GPs, community health; Maternal & Child Health • ‘Tier’ 2/secondary level services – private psychologists, AOD, homelessness services • Specialist MH services – state funded clinical and PDRS (NGO); private psychiatrists • Commonwealth funded services across the spectrum – system increasingly complex with risk of further fragmentation
Clinical (CAMHS, adult, aged) Inpatient beds PARC beds Secure Extended Care beds Community Care Units Forensic beds Community mental health teams (CAT, MST, CCT, PMHTs) PDRSS – psychiatric dis’y rehab & support services (non govt) Residential rehabilitation Supported accommodation Home Based Outreach at 2 levels IRRCS Day Programs Mutual Self Help & Support Koori program State funded specialist system
Legislative framework • 1986 Mental Health Act – increased transparency & accountability for patients predominantly in institutional settings • Statutory ‘watchdogs’ – Mental Health Review Board, Public Advocate; Chief Psychiatrist, Community Visitors, Ombudsman, Health Services Commissioner • Sentencing Act 1991 – restricted involuntary treatment orders & hospital security orders • Crimes (Mental Impairment & Unfitness to be Tried) Act 1997 – custodial & non custodial supervision • 2007 – Charter of Human Rights & Responsibilities – increasing community expectations on respect for rights; MHA + MHB policies & procedures being examined
Issues • Access – 50% of nominal client group being seen (60,000 clients per year) • High demand on beds – long waits in EDs (ALOS – 11 days) • High levels of complexity – dual diagnosis; other co-morbidities; growing proportion of involuntary (71% of admitted group) • Workforce shortages & maldistribution • Beyond health – housing, employment, social connection • Accommodating community safety as well as personal autonomy & rehabilitation/recovery
Recent service developments • Build the core and develop new service models • PARC • Youth early psychosis • CAMHS & Schools Early Action (conduct disorder) • Families where parents have a mental illness (FaPMI) strategy • Aged intensive community treatment (bed substitution)
New mental health strategy • Whole of government approach – IDC with Vicpol, DoJ, Education, Office for Children, Housing, Primary Health etc • Key areas under consideration – early intervention; access and responsiveness of system including for people in crisis, and system gaps for particular groups; family support; MH/AOD interface; justice interface; community participation
Justice system interfaces and issues • Diversion– relevant programs include - court liaison services – (DHS 1994) court based, provided by Forensicare in 4 metro & 5 rural courts – assessment; links to services - court integrated services program (DoJ2006 assistance; case man’t; pathways to service; joint DoJ/MHB project examining program • Neighbourhood Justice Centre – 2006; court; on site services; work with local community • All aiming to divert; achieve access to right care; reduce re-offending
Other developments • Community Corrections Protocol – under development; aims for a systematised approach for people in corrections system with MH problems or in need of crisis care Prisoner pathways and discharge plans • MH/Juvenile Justice & Community Corrections/COATs protocols are in place
Areas for further development • Diversion programs • Attention to pre and post release – risk of relapse & reoffending at transition – how can services work better & achieve continuity of care? • Core MH specialist service system resources and skills (clinical & PDRSS) • Required focus on the forensic group