Download
1 / 35
350 likes | 368 Views
An Overview of the Role of the Pharmacist in Pain Management. Sarah Walden, PharmD Kaweah Delta Medical Center Associate Clinical Professor of Pharmacy, UCSF. About Me (Quickly). UC Davis Graduate in 2010 Attended UCSF School of Pharmacy 2011-2015

E N D
An Overview of the Role of the Pharmacist in Pain Management Sarah Walden, PharmD Kaweah Delta Medical Center Associate Clinical Professor of Pharmacy, UCSF
About Me (Quickly) UC Davis Graduate in 2010 Attended UCSF School of Pharmacy 2011-2015 Post Graduate Year 1 (PGY1) Training at Kaweah Delta Medical Center (KDMC) Focus in pain management Hired on at KDMC to inpatient pain team Helped to build and recruit for outpatient pain clinic Currently involved in resident training, studentpreceptorship, policy building, order set revision, etc
About Me (cont.) Fell in love with pain management while shadowing at UCDMC Many rotations in pain management in both inpatient and outpatient setting GREAT things about working in pain management Going to be huge need going forward (“opioid epidemic”) Pain management is an area of pharmacy where you get to be really creative
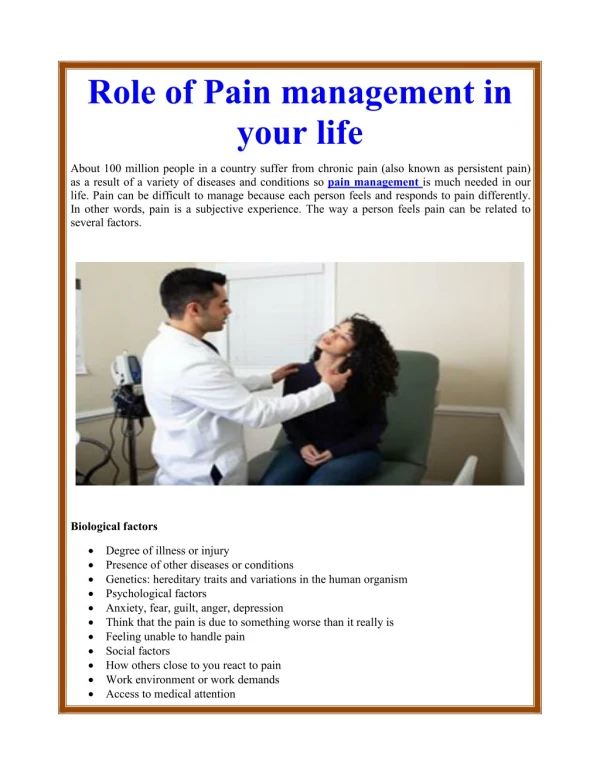
Why does pain matter?1 * Approximately 100 million adults in U.S. affected by chronic pain (including joint pain or arthritis) * Total financial cost of pain to society: $560- $635 billion Combines the health care cost estimates and the following three productivity estimates Days of work missed ($11.6 - $12.7 billion) Hours of Work Lost ($95.2 - $96.5 billion) Lower Wages (190.6 - $226.3 billion ) Results of 2008 Medical Expenditure Panel Survey (MEPS).
Why does pain matter?1 Annual Cost of pain was greater than the annual costs, in 2010 dollars, of the following: Heart Disease ($309 billion) Cancer ($243 billion) Diabetes ($ 118 billion) Note: Pain costs approx. 30% higher than combined costs of cancer and diabetes
Recent data2,3 Between 1997 and 2007, the number of opioid prescriptions increased 700% CDC reported 27,658 deaths secondary to unintentional opioid overdose in 2007.2 Approximately 1.4 million drug-related visits to emergency rooms throughout the country in 2011 420,000 visits were associated with opioid analgesics.
More statistics4 In 2013, there were 43,982 drug overdose deaths in the United States. Fifty-one percent (22,767) were related to pharmaceuticals agents. When this population was further sub-stratified: 16,235 (71.3%) were observed to have involved use of opioid analgesics.
Why does pain matter? Pain management is tied to the financial health of institutions. HCAHPS scores – measure patient satisfaction through a series of “domains” During this hospital stay, did you have any pain? During this hospital stay, how often did hospital staff talk with you about how much pain you had? During this hospital stay, how often did hospital staff talk with you about how to treat your pain? Focused on patient education - direct recommendation from Joint Commission after visit to our pain service in 2017
Challenges Facing Pain Management in the U.S. Healthcare System Current state of pain management education Healthcare culture Misperceptions facing the patient with pain
Understanding the State of Pain Education in the U.S.5 Utilized the Association of American Medical Colleges’ (AAMC) CurrMIT: Centralized, password-protected, repository of curricular information for US medical schools. 145 medical schools (in US and Canada) assessed. 104 US medical schools met criteria for inclusion in study (CurrMIT participants)
Understanding the state of Pain Education in the U.S.5 Pilot study (process of identifying search methods): it was discovered that pain education is provided in 1 of 3 routes: • Within sessions or topics of an elective course • Within another required course • Within a required course dedicated to pain
Findings5 Of 104 medical schools, 4 (3.8%) reported having a required pain course. Duration of course ranged 1.5-13 days Additional 17 offer a designated pain elective 8 of these offer more than 1 elective in pain education Cumulative number of pain teaching hours: 11.13 (±8.23) hours. Range 1-31
So now what? Pain is one of the most common complaints of people presenting for medical attention. As such, it is important to: Appropriately initiate analgesic use when indicated Tailor therapy specifically to the patient to minimize medications risks/adverse events.
The Pharmacist’s Role in Pain Management Pharmacists have unique training as medication specialists More knowledge of side effect profiles, correct usage, dosage, etc Understanding of how to target drug therapy for specific pain types Pharmacists have more time to counsel and help patients understand medication choices
Pharmacy Pain Management Service atKDMC 3 Full-time inpatient pharmacists 581 bed inpatient facility Time split between oncology + pain management 1 Stewardship/outpatient pain clinic pharmacist Focus on identifying patients at risk for adverse events, monitoring opioid usage, help with pain clinic 1 Full-time outpatient pain clinic pharmacist Sees 70+patients in clinic, writes scripts,makesreferrals
Inpatient Pain Service All types of pain from acute pain from surgery, trauma, chronic pain from old injuries/disease states, cancer pain, hospice and end of life care Focus on challenging patient cases Workflow Receive consult Work up patient, conduct interview Recommendations made to medical team Follow patient until pain controlled or patient discharged Referral to pain management clinic if needed
Reported pain score and objective observation Visual Analogue Pain Scales
Pain Assessment A number out of 10 is not the only way to assess pain There are lots of factors we look at to determine what types of pain a patient may be experiencing PQRST/AU
P – Palliative/Precipitating Factors Q – Qualitative (Dull, Sharp, etc.) R – Radiation (is the pain localized or transmitted elsewhere in the body) S – Severity (0-10/10) T – Time (when in day is pain noted) A – Associative (symptoms associated with pain) U – How does the pain affect YOU Assessing Pain6
Pain Subtypes6 Not all pains are created equally and thus are not treated the same. These pain subtypes include: Somatic Pain Visceral Pain Neuropathic pain
Somatic Pain6 Dull/aching pain Pain is well localized Commonly localized in skin and subcutaneous tissues. Less localized in bone, muscle, blood vessels, or connective tissue.
Visceral Pain6 Cramping/Sharp pain Poorly localized, diffuse, deep Often referred to dermatonal sites from sites distant from the source of pain Originates in internal organs or body cavity lining.
Neuropathic Pain6,7 Results of injury of peripheral nerves or persistently uncontrolled pain Sharp, burning, or shooting pain. May also resemble electrical shock and may be accompanied by weakness. Non-painful stimuli may cause pain (allodynia) or, An exaggerated pain response may result (hyperalgesia)
P – Palliative/Precipitating Factors Q – Qualitative (Dull, Sharp, etc.) R – Radiation (is the pain localized or transmitted elsewhere in the body) S – Severity (0-10/10) T – Temporal (when in day is pain noted) A – Associative (symptoms associated with pain) U – How does the pain affect YOU Assessing Pain6
Medication Options There are MANY! Take away point: Medication recommendations depend on description of pain COMMONLY missed in pain assessments Role of the pharmacist in pain management is to help to determine when to use an appropriate agent AND when to eliminate unhelpful or unnecessary agents
Goals6 It is imperative to set realistic goals of pain management with patient - A KEY function of our service line The goal of pain management is NOT to eliminate pain 100%. Goals of Pain relief initial decrease 3-4 points Improvement in activities/acceptably comfortable.
Recap LOTS of opportunities for pharmacists in pain management Can help make correct medication choices Can help set appropriate functional goals for pain patients Cheerleaders!
Where will you get involved in pain management? Shadowing at hospital sites - don’t be afraid to reach out to pharmacists Rotations in pharmacy school (IPPEs/APPEs) Come to the central valley! Post Graduate Training - PGY1 and PGY2 Residency 25 PGY2 pain/palliative care residencies listed on ASHP website now!
Thank you! Contact info: Sarah Walden, PharmD Kaweah Delta Medical Center 400 W. Mineral King Ave, Visalia, CA swalden@kdhcd.org Type to enter a caption.
References 1. Gaskin DJ, Richard P. The Economic Costs of Pain in the United States. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Washington (DC): National Academies Press (US), 2011.301-338 2. Boyer EW. Management of Opioid Analgesic Overdose. N Engl J Med 2012;367:146-155. doi: 10.1056/NEJMra1202561. 3. Substance Abuse and Mental Health Service Administration. The DAWN Report: highlights of the 2011 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. SAMHSA Website. Available from URL: http://archive.samhsa.gov/data/2k13/DAWN127/sr127-DAWN-highlights.htm. Accessed April 24, 2015 4. Centers for Disease Control and Prevention. National Vital Statistics System mortality data. (2015). Available from URL: http://www.cdc.gov/nchs/deaths.htm. Accessed April 24, 2015 5. Mezei L, Murinson BB, and the Johns Hopkins Pain Curriculum Development Team. Pain Education in North America Medical Schools. The Journal of Pain. Vol 12, No 12 (December), 2011: pp 1199-1208 6. McPherson, M.L. Demystifying Opioid Conversion Calculations. American Society of Health-System Pharmacists. 2010. 7. Dipiro, J.T., Talbert, R.L.,Yee, G.C., Matzke, G.R., Wells, B.G. et al. Pharmacotherapy: A Pathophysiologic Approach 6th Edition. Mcgraw-Hill 2005. 1089 – 1104 8. Perkins FM, Kehlet H. Anesthesiology 2000;93;1123-33 9. Dipiro, J.T., Talbert, R.L.,Yee, G.C., Matzke, G.R., Wells, B.G. et al. Pharmacotherapy: A Pathophysiologic Approach 6th Edition. Mcgraw-Hill 2005. 1089 – 1104 10. Macintyre PE, Schug SA, scott DA, et al 2010. Acute Pain Mgmt: Scientific Evidence (3rd edition). ANZCA and FPM, Melbourne 11. Grape S, Tramer MR. Nest Practice Res Clin Anaesthesiology 2007; 21(1):51-63 12. Hudcova J, McNicol E, Quah C et al. Cochrone Database Stsem Rev (2006 (4): CD 003348 13. Substance Abuse and Mental Health Service Administration. The DAWN Report: Benzodiazepines in Combination with Opioid Pain Relievers or Alcohol: Greater Risk of More Serious ED Visit Outcomes. (2014). Available from URL: http://www.samhsa.gov/data/sites/default/files/DAWN-SR192-BenzoCombos-2014/DAWN-SR192-BenzoCombos-2014.pdf. Accessed April 24, 2015 14 Johnson, S.J. Opioid Safety in Patients with Renal and Hepatic Dysfunction. www.pain-topics.org . June 2007