Download
1 / 113
1.13k likes | 1.13k Views
This unit of study aims to define and differentiate neoplasms and malignant disorders, compare and contrast different types of hematopoietic neoplasms, describe classification systems, laboratory methods, and prognosis, and explain the role of proto-oncogenes and oncogenes. It also covers the effects of radiation, treatment options, and laboratory features of various neoplasms.

E N D
23 Introduction to Hematopoietic Neoplasms
Learning Objectives—Level I At the end of this unit of study, the student should be able to: • Define and differentiate the terms neoplasm and malignant and identify hematopoietic disorders that can be included in each category. • Compare and contrast the general characteristics of the myelodysplastic syndromes (MDSs), myeloproliferative neoplasms (MPNs), and acute and chronic leukemias. continued on next slide
Learning Objectives—Level I At the end of this unit of study, the student should be able to: • Describe the World Health Organization (WHO) classification system used for MDSs, MPNs, the leukemias, and lymphoid neoplasms. • List the various laboratory methods used to classify the hematopoietic neoplasms. continued on next slide
Learning Objectives—Level I At the end of this unit of study, the student should be able to: • Compare and contrast the laboratory findings of the acute and chronic leukemias and myeloid and lymphoid leukemias. • Differentiate proto-oncogenes and oncogenes and summarize their relationship to neoplastic processes. continued on next slide
Learning Objectives—Level I At the end of this unit of study, the student should be able to: • Correlate patient age to the overall incidence of the hematopoietic neoplasms. • Explain the usefulness of immunological techniques, chromosome analysis, molecular genetic analysis, and cytochemistry in the diagnosis and prognosis of hematopoietic neoplasms. continued on next slide
Learning Objectives—Level I At the end of this unit of study, the student should be able to: • State the prognosis and survival rates of the hematopoietic neoplasms. • Define and differentiate proto-oncogenes and oncogenes.
Learning Objectives—Level II At the end of this unit of study, the student should be able to: • Explain how proto-oncogenes are activated, and the role that oncogenes and tumor suppressor genes and their protein products play in the etiology of hematopoietic neoplasms. • Describe the effects of radiation on the incidence of leukemia. continued on next slide
Learning Objectives—Level II At the end of this unit of study, the student should be able to: • Differentiate between the acute and chronic myeloid and lymphoid leukemias based on their clinical and hematologic findings. • Reconcile the use of chemotherapy for treatment of leukemia. continued on next slide
Learning Objectives—Level II At the end of this unit of study, the student should be able to: • Compare and contrast treatment options for the hematopoietic neoplasms, including possible complications. • Name the leukemogenic factors of leukemia and propose how each contributes to the development of leukemia. continued on next slide
Learning Objectives—Level II At the end of this unit of study, the student should be able to: • Compare and contrast laboratory features of MDS, MPN, acute myeloid and lymphoid leukemia (AML, ALL), and mature lymphoid neoplasms, and justify a patient diagnosis based on these features. continued on next slide
Learning Objectives—Level II At the end of this unit of study, the student should be able to: • Define the principles of, explain the applications of, and select appropriate cytochemical stains for bone marrow evaluation of hematopoietic neoplasms. • Select laboratory procedures appropriate for confirming cell lineage and diagnosis in hematopoietic neoplasms. continued on next slide
Learning Objectives—Level II At the end of this unit of study, the student should be able to: • Define epigenetics and define its role in cancer. • Define cancer stem cell and explain its similarities to the hematopoietic stem cell (HSC).
Introduction • Neoplasm • "New growth" • Dysregulated proliferation • Genetic mutations • Benign or malignant ("cancer") • Neoplasms of hematopoietic cells • Lymphoid or myeloid • Premalignant and malignant neoplasms
Figure 23-1 The spectrum of hematopoietic proliferation ranges from benign to malignant outcomes. Benign myeloid and lymphoid proliferation is usually a reactive process (reactive leukocytosis; leukemoid reaction). Mature myeloid and lymphoid neoplasms include myeloproliferative neoplasms (MPNs), and myelodysplastic syndromes (MDSs), chronic lymphocytic leukemia (CLL), and plasma cell neoplasms. These neoplasms are derived from a mutated precursor cell that divides incessantly but has some capacity to mature. Acute leukemia (AL) is a malignant precursor neoplasm characterized by unregulated cell proliferation and a block in maturation. Mature neoplasms can progress with additional genetic mutations and terminate in AL.
Introduction • Leukemia • Malignant neoplasm of bone marrow • Lymphoid, myeloid, histiocytic/dendritic • Myeloid and lymphoid subgrouped as: • Precursor (acute) neoplasm • Mature (chronic) neoplasm
Table 23-1 Comparison of Precursor and Mature Hematopoietic Neoplasms
Acute Leukemias • Precursor neoplasms • Characterized by genetic mutations that promote proliferation and survival and/or block differentiation into mature cells
Acute Leukemias • Acute leukemia has leukemic hiatus. • Gap in the normal maturation of cells with many blasts, some mature forms • Arise from residual normal HSCs in the BM, but ↓ in intermediate maturational stages
Figure 23-2 Acute myeloid leukemia. Note the large number of myeloblasts with no mature granulocytes present (Wright stain, 1000× magnification, peripheral blood).
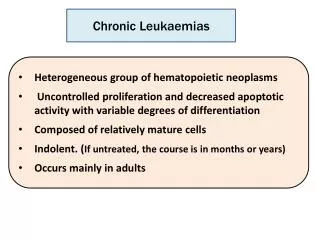
Introduction • Mature neoplasms • ↑ in proliferation and survival of neoplastic cells • Maturation progenitor cells nearly normal • Leukocytosis • Predominant leukemic cells amitotic, mature, normal function • May exhibit dysplastic features
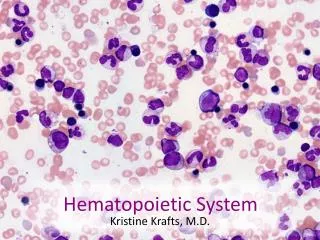
Figure 23-3 Chronic myelogenous leukemia. Note the large number of granulocytic cells in various stages of maturation including blasts, metamyelocyte, bands, and segmented neutrophils (Wright stain, 1000 magnification, peripheral blood).
Introduction • Lymphoma—abnormal proliferation lymphoid cells in lymphatic tissue or lymph nodes • Solid tumors • When affects BM, lymphoma cells found in peripheral blood, considered the leukemic phase of lymphoma
Figure 23-4 Clonal expansion of neoplastic cells in the bone marrow over a period of time leads to a decrease in the concentration of normal cells in both the bone marrow and peripheral blood.
Etiology/Pathophysiology • Cancer initiating cell • Genetic mutation • HSC or differentiated progenitor cell • Capacity for unlimited self-renewal • Gives rise to cancer stem cell
Etiology/Pathophysiology • Cancer stem cell • Generate identical clones and sustain malignant growth • Heterogeneous cell populations • Chromosomal alterations (+/− abnormal karyotype) • DNA alterations at the molecular level
Figure 23-5 A hematopoietic neoplasm (left) is derived from a single cancer-initiating cell. The leukemic mutation(s) (black arrows) that transform a normal hematopoietic precursor cell to a cancer-initiating cell can occur at the hematopoietic stem cell (HSC) or more committed progenitor. If the cancer-initiating cell is a committed progenitor, then the mutations must include the capacity for self-renewal (blue arrows). If the mutation also can result in a block to terminal differentiation ( ) the resulting malignancy will be an acute leukemia (AL). Residual "normal" HSCs and committed progenitors in the marrow will still be capable of producing mature cells (right).
Oncogenes • Oncogene • Altered cellular gene that can cause cancer/tumors; plays role in cell cycle • Proto-oncogene • Normal, unaltered cellular counterpart of oncogene • Regulates initiation of DNA replication, cell division, commitment to cellular differentiation and/or apoptosis
Oncogenes • Oncogene activation • Structural mutations • Result in continuous activity of protein or production of protein at wrong time or place
Oncogenes • Proto-oncogenes serve functions in normal cell growth: • Growth factors • Growth factor receptors • Signal transducer molecules • Transcription factors (nuclear)
Oncogenes • Proto-oncogene activation • Gene mutation, gene rearrangement, or gene amplification • Results in: • Enhanced activity of gene • Protein product no longer under normal regulatory control • Cell proliferates without normal controls (↑ production for quantitative change)
Tumor Suppressor Genes • Function is to inhibit cell growth in normal cells. • Tumor suppressor mutations are loss of function mutations.
Table 23-2 Properties of Oncogenes and Tumor Suppressor Genes
Epigenetics • Stable, heritable changes in gene expression, NOT due to changes in DNA sequence • Changes important in normal development and differentiation • Associated with "silencing genes" and chromatin condensation into heterochromatin
Epigenetics • Passed from one cell generation to next during mitosis
Epigenetics • Major epigenetic changes • DNA methylation of CpG dinucleotides • Histone acetylation/deacetylation reactions
Cell-Cycle Checkpoints and Cancer • Common features of cancer cells • Loss of regulation of cell-cycle checkpoints • Through overexpression of positive regulators (cyclins, Cdks) • Loss of function of negative regulators (p53, Rb, Cdk inhibitors)
Figure 23-6 Alterations of the G1 checkpoint that can lead to malignancy. Loss-of-function alterations in cell cycle negative regulators (i.e., the tumor suppressor gene products p16 or Rb) can contribute to uncontrolled proliferation. Similarly, gain-of-function mutations of positive regulators of proliferation can contribute to uncontrolled proliferation (i.e., the proto-oncogene gene products Cyclin D, Cdk4). = inhibition of the pathway; + = an alteration that increases activity of the indicated proteins; −=an alteration that decreases activity of the indicated proteins
Apoptosis and Cancer • Mutation of genes important in regulating apoptosis have been identified as oncogenes and tumor suppressor genes. • Includes loss of function mutations initiate apoptosis (p53, Bax, Bcl-2 family members) continued on next slide
Apoptosis and Cancer • Mutation of genes important in regulating apoptosis have been identified as oncogenes and tumor suppressor genes. • Results in production of cells with extended life span, ↑ proliferation capacity, diminished cell death continued on next slide
Leukemogenesis • Several factors play role: • Genetic susceptibility • Somatic mutation • Viral infection • Immunologic dysfunction • Miscellaneous factors
Leukemogenesis • Genetic susceptibility • Hereditary factors and abnormal genetic material have leukemogenic effects. • Increase risk of developing acute leukemia • Potential to activate proto-oncogenes or eliminate function of tumor suppressor genes (TSGs) • Example: Down syndrome
Leukemogenesis • Somatic mutation • Acquired change in the genetic material of cells other than those involved in reproduction • Radiation, chemicals, drugs cause mutations continued on next slide
Leukemogenesis • Somatic mutation • Chromosome breaks and translocations lead to oncogene activation to aberrant expression of protein product. • Can produce hybrid genes with new protein products
Leukemogenesis • Viral infection • Unclear how viruses cause leukemia • Suspected that viral genome incorporated into host DNA through retroviruses • Activates proto-oncogenes
Leukemogenesis • Immunologic dysfunction • Congenital and acquired immunologic disorders • Could be due to breakdown in cell • Mediated immunologic self-surveillance system • Production of antibodies against foreign Ags leading to neoplastic cells
Leukemogenesis • Miscellaneous factors • Hematologic diseases • No single factor, includes genetic factors and environmental exposures
Epidemiology • Most cases occur in older adults • > ½ occur after age of 67 • ~ 50% are diagnosed as acute continued on next slide
Epidemiology • Variations in leukemia among age groups • Acute leukemia occurs at all ages. • Peak incidence in the first decade • Decrease incidence in second and third decade • Begins to rise, rises steeply after age 50
Table 23-4 Age Groups Typically Found in Acute (Precursor) and Chronic (Mature) Leukemias