Download
1 / 20
200 likes | 309 Views
Respiratory Physiology Diagnostics North East Glasgow. Roger Carter Consultant Clinical Scientist. The service we provide :. The North East Glasgow Hospitals provide lung function service to a local population of 350,000

E N D
Respiratory Physiology DiagnosticsNorth East Glasgow Roger Carter Consultant Clinical Scientist
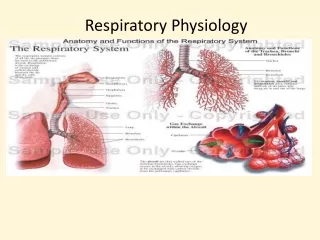
The service we provide : The North East Glasgow Hospitals provide lung function service to a local population of 350,000 A wide range of diagnostic respiratory physiology services are delivered from two dedicated respiratory physiology laboratories based at Glasgow Royal Infirmary and Stobhill Hospital . In total 42 respiratory/ sleep investigations have been coded : The following investigations are offered at both sites: • Spirometry ** • Bronchodilator Assessment** • Lung Volumes by Body Plethysmography • Transfer Factor and components • Ear lobe capillary blood gases • LTOT Assessment • Ambulatory Oxygen Assessment • Flight Assessment • Bronchial Reactivity • Cardio-Pulmonary Exercise Testing • Surgical Risk Assessment • Nebuliser Assessment • Nebuliser Exchange Service • Outreach Spirometry (GP Flow Volume Loops)** • Respiratory Muscle Assessment • Respiratory Drive • Sniff Pressures
FEV1 Volume (Litres) Normal Obstructive Restrictive Severe Obstruction Time (Seconds) Volume Time Curves
Diagnosis of COPD EXPOSURE TO RISK FACTORS SYMPTOMS cough tobacco sputum occupation dyspnea indoor/outdoor pollution è SPIROMETRY
NICE COPD 2004: Severity of obstructionFEV1/FVC <70% FEV1 <80% >=50% Predicted: Mild airflow obstruction FEV1 <49% >=30% Predicted: Moderate airflow obstruction FEV1 <30% Predicted: Severe airflow obstruction
Diagnosis: Asthma • The diagnosis of asthma is based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative explanation for them. • If high probability - trial of treatment • Low/Moderate - attempt to find airflow obstruction (Spirometry with reversibility to acute bronchodilator administration)
Intermediate Probability of Asthma • In view of lifelong treatment seek objective evidence of airflow obstruction • Spirometry is preferred over peak flow at diagnosis • Caveat - normal spirometry if asymptomatic does not exclude asthma • Peak flow diaries demonstrating airflow variability are helpful
Symptoms Smoking cessation 100 Healthy population Antibiotics for acute infections 80 Smokers cough Little or no dyspnoea No abnormal signs Trial Symptomatic bronchodilator therapy Worsening lung function Trial Long acting Bronchodilators Inhaled steroid if freq exacerbations 60 Exertional dyspnoea Cough & sputum Some abnormal signs Influenza vaccination Pulmonary rehabilitation FEV1 as % predicted Assessment for LTOT 40 Dyspnoea on mild exertion Hyperinflation & cyanosis Wheeze & cough 20 Death Increasing investigation and treatment Management of stable COPD
Waiting Times: Spirometry • 2007 • Average Waiting Time 9 weeks • Longest Waiting Time 12 weeks
Make a difference by : • Introduction of efficient administrative systems to manage the booking system more effectively and improve local pathways. • Reduction of waiting times by actively managing the booking of diagnostic respiratory tests and the use of first available spirometry slot at any north east site.
Making a difference: what we did : • Previously appointments for the service were booked onto a paper diary list by an assistant technical officer. • We have developed electronic clinic templates for Respiratory Diagnostic testing on the PAS system. • These are, at present, appointed by clinical physiologists. • This has enabled: • Flexible booking system - better time management relative to the type of tests and specialty clinics. • Record accurate data on patient administration system. • Owing to the complexity and time consuming nature of some of the investigations, short notice patient cancellation or non-attendance are particularly wasteful of resources and this can occur on a regular basis. Patients who cancelled appointments were regularly offered repeat appointments, increasing the length of the waiting list and reducing the availability of slots. • The administrative team actively applied the health board’s waiting list policy so that patients who do not attend or cancel their appointment twice are removed from the waiting list and returned to their referrer with an explanation of the action. Also patients who decline two or more reasonable notice appointments, but still wish to be investigated, are clearly flagged under patient choice and do not reflect in the waiting list statistics.
What benefits did we achieve? • Streamlined patient booking pathway therefore better patient experience. • The ability to offer first available appointment at either laboratory (two laboratories but single service) if the patient was prepared to travel or the most appropriate site at the patient’s request • Reduced number of patients arriving without referral forms and patients are better informed (Clinical Portal Access) • Flexible booking times – increased capacity for one-stop clinics. • A reduction in cancellations and DNAs. • A reduction in waiting times. • Involvement in the Diagnostic Working Group to review the waiting list policy and the inclusion of diagnostic services in to the waiting list policy (DMMI) • Improved staff awareness of current waiting lists and activity through the publication, by the department manager, of monthly statistics.
How we measured the achievement? • Data analysis from PAS. • Reduced waiting times for new patients from 9 weeks to approximately 4 weeks. • Increased one-stop clinics due to better time management by physiologists. • Reduced waiting times were observed in the monthly returns • Tables indicating the waiting time trends and including activity, referral and patient DNAs.
Example Table: Number of patients waiting, listed by period, since the date orv receipt of referral for the test, as at last day of the month: SPIROMETRY
What challenges did we face in making this idea work for us? • The transfer of appointments from the paper diary to the PAS system involved a concerted effort of clinical physiologist time. • Natural scepticism of clinical physiologist staff in initiating this booking system and the move away from a paper diary • Training the clinical physiologist staff to manage our investigation bookings in line with additional information being provided by the waiting list tables, whilst still maintaining a sensible rationale for patients with different indicated clinical urgency. • Ensuring all multiple cancellation and DNA patients were managed in accordance with the Trust waiting list policy and where there was any ambiguity to discuss each case with the Consultant Clinical Scientist
Further Development • A dedicated administrator appointment to manage patient bookings: • Freeing of clinical physiologist time presently spent on doing routine administrative tasks to perform respiratory diagnostics with a proposed further fall in waiting times. • Introduction of electronic booking of respiratory diagnostic tests through the clinical portal with associated reduction in paper referrals and reduction in time spent in obtaining referrals through the internal mail. • Scoping of all respiratory physiology/sleep diagnostic tests (42 in total) to address 18 weeks RTT